Beyond Blame, our flagship meeting for activists, human rights defenders, criminal legal system and public health system actors, healthcare professionals, researchers, and anyone else working to end HIV criminalisation, is returning for a special eve-of-World AIDS Day edition.
Beyond Blame is a unique opportunity to learn why HIV criminalisation matters, as well as hear about the wide range of initiatives and strategies that have been used by activists, lawyers, networks, and organisations around the world to work towards ending the inappropriate use of criminal law to regulate and punish people living with HIV.
We will be highlighting some of the successes and challenges of the global movement to end HIV criminalisation over the past year, including work on ending the criminalisation of women living with HIV for breastfeeding, exploring whether scientific advances, such as the prevention benefit of treatment (U=U) and Molecular HIV Surveillance, help or hinder our movement and much, much more.
Beyond Blame will take place in English, with interpretation available in French, Russian and Spanish.
A new briefing paper published today by Positive Women’s Network-USA on behalf of the HIV JUSTICE WORLDWIDE coalition aims to support people living with HIV, activists, legal experts, and human rights campaigners in understanding the complexities and consequences of molecular HIV surveillance (MHS).
“Molecular HIV Surveillance: A global review of human rights implications” provides a detailed explanation of what MHS is and how it is used across the globe, including how the technology works, where it is being conducted, and by whom. The paper describes growing human rights concerns relating to the use of this technology and goes on to list a number of recommendations for the use of MHS which were gathered from an international literature review and from members of the Expert Advisory Group.*
Molecular HIV surveillance (MHS) is an umbrella term that describes a wide range of practices focused on the monitoring of HIV variants and the differences and similarities between them for scientific research, public health surveillance, and intervention.
To conduct MHS, scientists rely on the results of HIV genetic sequencing tests taken from people living with HIV – these tests are often done before prescribing HIV medication to determine if the individual has a strain of HIV that is resistant to certain treatments. Interest in, and use of, MHS for reasons other than tailoring treatment regimens is increasing globally, however. Of particular concern, in some regions, MHS is being conducted and HIV data is being shared in ways that put the rights and safety of people living with HIV in jeopardy.
“HIV is highly stigmatised and communities that are most vulnerable to acquiring HIV are already highly policed and at risk for violence” said Naina Khanna, co-executive director of Positive Women’s Network-USA, a US-based membership organisation led by women and people of transgender experience living with HIV. “In more than 30 states in the US alone, and over 100 countries around the world, people with HIV can be criminalised on the basis of their health condition. Taking this kind of data from people without their consent or knowledge and storing or sharing it without adequate protections is extremely risky and could come at the cost of someone’s personal safety, their livelihood, and in the case of HIV criminalisation, their freedom.”
The paper highlights how HIV experts and advocates have raised a range of human rights concerns about this technology. These include:
Consent and autonomy;
Lack of community consultation;
Increased stigma on targeted communities;
Privacy and data protections;
Whether or not the technology can be used to “prove” direct transmission; and,
How MHS may intensify HIV criminalisation within communities who are already marginalised and oppressed.
Edwin J Bernard, Executive Director of the HIV Justice Network and global co-ordinator of the HIV JUSTICE WORLDWIDE coalition added: “MHS treats people living with HIV as ‘clusters’ and targets of public health interventions, rather than the beneficiaries of public health. When you combine MHS with HIV criminalisation it’s a perfect storm. That’s why I commissioned PWN-USA to produce this briefing paper as a first step to understand the problems and to suggest a range of possible solutions. With increased knowledge on the practices of MHS, individuals and organisations can be better equipped to advocate for ending research and surveillance practices that have the potential to harm the rights, autonomy, and well-being of people living with HIV.”
The paper provides wide-ranging recommendations for change aimed at various stakeholders, highlighting five key areas of action:
Take seriously and act upon community concerns about MHS.
Respect the bodily autonomy and integrity of people living with HIV in all our diversity.
MHS implementers must demonstrate a clear public health benefit that outweighs the potential harms of MHS, including by ensuring protections (i.e., data privacy, legal protections, social harms prevention, etc). These demonstrated benefits of MHS must measurably include people living with HIV.
Providers ordering HIV sequencing must inform people living with HIV about how their blood and data are being used for MHS purposes and be allowed to withdraw the consent if they so wish, without fear of negative consequences to their HIV treatment and care.
Implementers of MHS should publicly advocate against punitive or coercive laws and policies aimed at people living with HIV and ensure that MHS is never used in criminal, civil, or immigration investigations or prosecutions.
Follow the online conversation on Twitter by using the hashtags #EndMHS #DataPrivacy #DataProtection #HIVJustice and by following @HIVJusticeNet@uspwn.
We gratefully acknowledge the financial contribution of the Robert Carr Fund to this report.
The proverb says, “It takes a village to raise a child”. But what if a mother in the village is living with HIV, and some of the villagers stigmatise her? What if that stigma creates a situation where the mother living with HIV is unjustly criminalised because of her HIV status? Then it takes more than a village to get justice for that woman. It takes a global movement to end HIV criminalisation to sensitise and train lawyers and expert witnesses. It takes national communities of women living with HIV to support that woman following her release, and to educate the community in which she lives about HIV.
Introduction
In 2016, a Malawi court convicted a woman living with HIV of “negligently and recklessly doing an act likely to spread the infection of any disease which is dangerous to life” under section 192 of the Malawi Penal Code. She had attended a village meeting with her baby which she breastfed as usual before passing the child to her grandmother. Another woman then asked her to hold her baby. It was alleged that this child began breastfeeding briefly before the woman realised what was happening. The child’s mother then reported the incident to the police. The woman was arrested and without legal advice or representation, pleaded guilty, was convicted, and sentenced to nine months’ imprisonment with hard labour.
In addition, the accused woman was taking antiretroviral therapy. The chances of HIV transmission through even long-term breastfeeding are very low (which is why WHO guidelines recommend it when access to infant formula and clean water are limited) and the chances of transmission during the brief period the baby allegedly fed were infinitesimally small. In fact, the accused woman’s own child, who was routinely breastfed, has not acquired HIV, calling into question any suggestion that she intended to cause harm to the other woman’s child. Perversely, for a system that unjustly condemned her for risking harm to the other woman’s child, her own baby was imprisoned with her, without any arrangements for appropriate feeding and care, negating any notion that the legal system’s purpose was to protect children.
Following media reports of her initial conviction, numerous individuals and organisations – including HJN and our HIV JUSTICE WORLDWIDE partners, ARASA and SALC – became involved in the case, ultimately changing the outcome for the woman and her family, and laying the groundwork for further anti-HIV stigma advocacy and education in the region. Her story demonstrates the vital role that education, training, strong networks, and community play in the pursuit of HIV justice.
Living with HIV-related stigma
When interviewed at her home in 2019, the woman referred to as “EL” talked about her life:[1]
[1] The initials EL are used instead of her full name following a court order of anonymity to protect her privacy. The interview took place in 2019, during the village visit described later in this article.
“As kids, there were the two of us — me and my brother. My parents faced challenges raising us. Finding the basic necessities like soap and food was a tall order, let alone talking about going to school. It was difficult to get learning materials as well as proper clothes to wear at school. I worked hard in class but couldn’t get past Standard 5 at primary school. Eventually I dropped out, and my brother did the same, … My daily life was taken up doing house chores just like any other girl in the village, as well as helping my parents with farming. At 16, I got married.”
EL further described how she was diagnosed HIV-positive in 2015 after a de facto compulsory HIV test at an antenatal visit. She already had two children and was pregnant with her third. She had heard about HIV but did not know much about it. EL said that the healthcare workers provided a lot of assistance, giving her accurate information about HIV, including the importance of adhering to her antiretroviral treatment (ARVs).
EL and two of her children. Photo: Amos Gumulira/UNDP Malawi
EL said that she generally enjoyed life in her village, although at times she was subject to stigma and discrimination:
“When I went to fetch water at the community borehole, people would laugh at me, and whenever I wanted to participate in community work, you would find pockets of community members talking ill about me. Some people used to insult me, calling me names. But I persevered because my relatives, including the Village Headman himself, gave me support and always stood by my side.”
Members of EL’s family also faced discrimination. “Due to lack of information, a lot of people thought HIV was hereditary and because I was diagnosed HIV-positive, this meant that all my family members had HIV, and they were discriminated against,” EL said.
EL wonders if more could have been done to help her fight stigma. In particular, EL gained a lot of knowledge about HIV from the counselling she got when diagnosed, but perhaps she could have been better equipped with information to share with people in her community:
“A lot of people don’t know that if you adhere to ARVs, you reduce the risk of transmitting HIV to others. This information needs to be passed on to many people. There are also other issues to do with ARVs. A lot of people don’t have adequate information on the effects of ARVs and at the end of the day, they start pointing fingers at each other, giving people room to start speculating about issues to do with witchcraft.”
EL’s prosecution had repercussions for her whole village. One woman from the community explained:
“I was there and very close to where EL was sitting. Yes, she was carrying another woman’s child. This other woman had given the child to EL for safe keeping while she went to stand in a queue, but honestly speaking, I didn’t see EL breastfeed the child. I just heard some people who were sitting a distance from where we were sitting, as they started pointing accusing fingers at her.”
She said that things moved so fast that before they could think of anything to stop what she called “the rumour.” It had gotten out of hand and people started saying that EL had intentionally breastfed the child to transmit HIV.
After receiving a summons, EL voluntarily turned herself in at the police station. She was accompanied by the Village Headman (her grandfather) who wanted first-hand information about what crime she was alleged to have committed. That same day, police transferred EL to a larger town, where she was remanded for three days. At the age of 29, this was the first time that EL had ever left her village.
Days later, she appeared in court and the charge sheet was read out. EL recounted that she had not understood what was happening and could not make arguments because she had no legal representation. EL agreed with the summary of events as they were described, so she was found guilty and was imprisoned together with her youngest child.
She described life in prison as “hell”:
“After a week, my brother showed up to give me my ARVs. All this talk about a woman with HIV breastfeeding. I breastfed but I also found it tough to feed my baby while in prison because there was no provision of special food for babies. We were eating nandolo (pigeon peas) almost every day with Msima ya Mgaiwa (maize meal). And there was only one toilet for a cell of more than 50 people.”
After some time, relatives and other members of her community started visiting, giving her money she could use to buy soap and food for her baby. “When we heard from our Village Headman that she had been arrested, we were so devastated”, a woman from EL’s village explained. “We raised funds for some members to go and give her support only to learn that she had been transferred to one town, then another, but some of us did manage on several occasions to visit her and offer our support when she was in prison.”
Then, out of the blue, EL received a message that some people had come looking for her. She went to meet them: a lawyer, Wesley Mwafulirwa, and his paralegal. They explained why they were there and asked if she would like them to appeal on her behalf. She accepted enthusiastically. “I was excited but at the same time I was confused because I could not believe that I could be so lucky to have these people come to help me.”
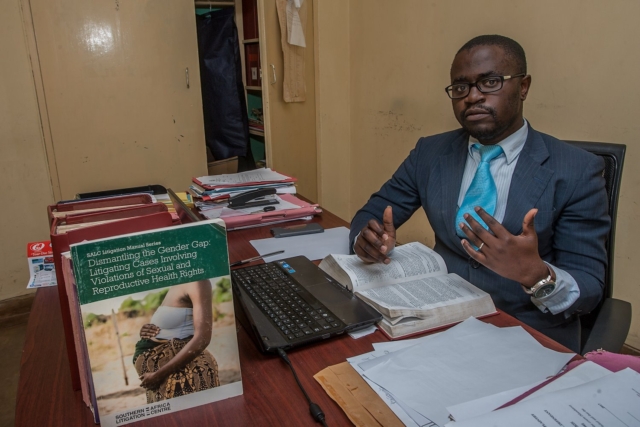
Fighting the charges
Solicitor Wesley Mwafulirwa had volunteered to attend training to address legal barriers to prison health and human rights presented by the Southern African Litigation Centre (SALC). He travelled from Malawi to South Africa to attend the training which addressed useful regional and international mechanisms, and presented insights about legal practice and strategic litigation to support prison health and human rights, particularly for those facing heightened vulnerability to HIV and TB.
At the training, two lawyers spoke about their pro bono work. Wesley remembers one of them, Allan Maleche (Executive Director of KELIN), saying that each participant should take at least one case when they go back to their country. It was a turning point in Wesley’s career.
He had not been home long when he saw an article in the newspaper about an HIV-positive person convicted for trying to spread HIV. That person was EL.
Wesley, who lives in a small town in northern Malawi, drove for more than ten hours to get to the jail where EL was incarcerated. He explained his determination, saying “I was so fired up! I’d just come from SALC’s training … and I said, ‘I want to take up this case’.”
Wesley interviewed EL and offered to take her case pro bono. Wesley contacted SALC, who offered technical support. Their first step was to get an order for anonymity to protect EL’s identity and gain greater control over media reporting. Next, they faced an ethical question. They wanted to challenge the constitutionality of the law but that would take a long time. Because EL was in prison, they decided to undertake a criminal appeal instead. They applied for EL to be let out of custody on bail pending appeal. This is usually a difficult application to win, but they were successful and EL was released from prison.
In the appeal, the court was asked to consider whether the conviction could be justified, whether the penal provision was constitutional (arguing it was overly broad and vague), and whether the sentence was manifestly unjust. Wesley used his learnings from the SALC training to raise international principles and instruments relating to sentencing, which the court referenced and upheld. Michaela Clayton, then Executive Director of the AIDS and Rights Alliance for southern Africa (ARASA), and now a member of HJN’s Supervisory Board, provided expert testimony. Another expert witness, Dr Ruth Brand, identified through HJN’s global network, gave expert scientific evidence to show the risk of HIV transmission had been “infinitesimally small.”
The case was heard by Honourable Justice Zione Ntaba, who held that the proceedings in the trial court were irregular and “blatantly bias” against EL, compromising her right to a fair trial. Justice Ntaba found the charge sheet had been defective and therefore EL’s plea should not have been recorded as guilty. She noted the law must be sensitive to the accused’s knowledge or belief (or lack of) that HIV would be transmitted. Justice Ntaba decided the conviction could not be justified, acknowledging human rights principles against the overly broad criminalisation of HIV non-disclosure, exposure, or transmission. EL’s sentence was set aside. (The Constitutional challenge was referred to a full-member panel of the Constitutional Court although the case was not pursued.)
Notably, Justice Ntaba was a member of the African Regional Judges Forum to discuss HIV, TB and Human Rights (a process which is owned and planned by the judges and run with support from UNDP and funding from the Global Fund).
Fighting the stigma
Shortly after EL’s arrest, the Coalition of Women and Girls Living with HIV and AIDS in Malawi (COWLHA) and the Malawi branch of the International Community of Women Living with HIV/AIDS (ICW-Malawi) discussed the case at a roundtable meeting. At first, everyone was surprised and even laughed, questioning how she could have breastfed someone else’s child. They had never heard of a criminal case involving infant feeding and did not understand what they were dealing with.
During their discussions, COWLHA and ICW-Malawi agreed that the prosecution of EL was a manifestation of stigma and misinformation about HIV in the community. They learned more about the unjust measures that EL had experienced, like being imprisoned without being given a chance to be heard and not being given the chance to prepare and take her medication and things she needed to care for her child. COWLHA and ICW decided to get involved.
Representatives from COWLHA and ICW meet with members of EL’s village. Photo: COWLHA/ICW
Concerned that EL could face social and community hostility after her release, COWHLA and ICW planned a visit to the village to provide psychosocial support to EL and to work with traditional community leaders to provide community sensitisation on HIV, addressing issues of stigma and discrimination. Their efforts helped change some community members’ ideas about HIV.
The community formed two support groups— one for youth and another for adults (notably both were predominantly female groups). They have conducted numerous activities, including home visits, supporting children to go to school, helping the elderly with house chores, and they have a garden where they grow vegetables and rice. They hoped to access loans to become self-reliant. They also had a list of issues they wanted to learn more about, including preventing mother-to-child transmission, sexual and reproductive health, positive living, stigma and discrimination, and treatment literacy.
Visiting EL at home
In September 2019, a three-member team comprising Edna Tembo (Executive Director of COWLHA), Charity Mkona (ICW Board Chair), and Peter Gwazayani (media consultant), set out for EL’s village.
The team was welcomed by the Group Village Headman, who took them to EL’s house. EL recognised Edna from the work COWLHA and ICW-Malawi had done in the community previously. EL welcomed the team with a big smile.
EL and her husband looked cheerful as they laid a mat on the veranda of their house for the visitors. Her mother later joined the discussion.
EL was interested to learn that HJN wanted to write about her case and the type of interventions that had been helpful, to share the story with advocates for HIV justice around the world.
EL recounted that when she returned to the village, “most members of my community received me with happiness, particularly my relatives. The day I arrived, they were jubilant. They celebrated with songs that we normally sing during special occasions in the village.”
COWLHA ED Edna Tembo and Charity Mkona of ICW chat with EL, her husband and her mother (at far distance). Photo: COWLHA/ICW
EL lives with her husband, five children and her mother in a compound made up of three grass thatched houses. She introduced her children:
“The oldest is 13 and she goes to school, as do the second and third. The fourth, a little girl, is the child I was with in prison. She has not yet started school. And then there is this one, who I am breastfeeding. She is the fifth one. She has been tested for HIV on two occasions and will be going for the last test soon. The other two tests have come back HIV-negative.”
EL’s accuser and her family still lives in the same village which has presented some difficulties. EL said that on several occasions she had tried to greet them when they passed each other, but she had been ignored. “They don’t talk to me but from deep down in my heart, I have no grudges against them,” EL said. “I am just living my normal life,” EL says, although now she says that she would never agree to carry anybody else’s child, for any reason.
Moving beyond criminalisation
With respect to the community-level interventions, lawyer Annabel Raw, who worked at SALC during the time they supported the EL case said:
“As lawyers, we would never have thought to consider such an intervention had ICW-Malawi and COWLHA not shared their insights and been willing to support the client and her community. Their work has been so important to ensuring that meaningful justice was done to combat the actual root cause of the prosecution — stigma and discrimination — and to reconcile EL with her community.”
Engaging with the community also influenced ICW-Malawi and COWLHA’s thinking about HIV criminalisation. COWLHA’s Edna Tembo noted that:
Supporting people who have been prosecuted, particularly women, gives them power, … However, it is very important to stress that psychological support is absolutely vital for those who have been prosecuted. That includes family support, and a supportive community environment enabling acceptance of an individual accused.”
Tembo was also quick to emphasise that there is more work to be done. That work includes awareness raising and ongoing support to the community, especially to identify and train volunteers, empowering them to provide services at community level and to link them to health facilities and district offices for continued support and mentorship.
EL carries her youngest child home. Photo: Amos Gumulira/UNDP Malawi
EL described her dreams for the future:
“My wish now is to see my children progress in school so that they become productive citizens in this community and help it grow. That’s my dream. If they get educated, they will be able to stand on their own and support others. My husband is not employed and it is a challenge to get money for school fees for our children. We would love to get a loan or training to have greater knowledge of economic empowerment because we want to be self-reliant. We would then love to lease some land to grow rice to sell to pay back the loan.
“It’s also my wish to see the lives of all people in the community uplifted. We farm but on a small-scale. If we were to be supported with funds, I’d love to see the community establish big rice farms, working in groups, harvesting for consumption and for sale. In so doing, we would be able to uplift our lives for the better.”
Further Information
Learn more about Wesley’s experiences in EL’s case here and here.
Learn more about the African Regional Judges Forum here.
The full High Court judgement is available here, with a summary included here.
Read more about the successful HIV and AIDS Management Act community advocacy here.
This article is based on information provided by ICW-Malawi and COWLHA following their visits to EL’s village, and an interview with Wesley Mwafulirwa published by UNDP. HJN provided financial and logistical support for the village visits thanks to a grant provided to the HIV Justice Global Consortium from the Robert Carr Fund for civil society networks.
“We want a people’s vaccine, not a profit vaccine”
Yesterday was the Global Day of Action for a #PeoplesVaccine.
On 11 March, one year since the World Health Organisation declared a COVID-19 pandemic, influential leaders including Winnie Byanyima from UNAIDS and social justice organisations like Human Rights Watch, joined tens of thousands of individuals and organisations all over the world demanding a People’s Vaccine – a vaccine that is made freely available to everyone, everywhere.
Countries in the global South are currently unlikely to receive a COVID-19 vaccine until 2023. This is a scandal and threatens everyone.
In a feature story published yesterday, UNAIDS highlighted that as developing countries are facing critical shortages of oxygen and medical supplies to cope with COVID-19, few have been able to administer a single dose of a COVID-19 vaccine. In contrast, rich nations have vaccinated their citizens at a rate of one person per second over the last month.
We wholeheartedly support this campaign to pressure pharmaceutical companies and governments to end vaccine monopolies. Following yesterday’s WTO vote by rich countries against waiving patent rules, we stand in solidarity with its demands that:
Governments suspend patent rules at the World Trade Organisation on COVID-19 vaccines, treatments, and testing during the pandemic. This will help break Big Pharma monopolies and increase supplies so there are enough doses for everyone, everywhere.
Click the link below to learn more about how you can support the People’s Vaccine campaign.
An editorial published to coincide with Zero Discrimination Day (March 1) by leaders in the HIV Justice movement celebrates “the courage and commitment of the growing global community of advocates, human rights defenders and others around the world who are challenging laws, policies and practices that inappropriately and unjustly criminalize people living with HIV”, but warns that this work must include and benefit those populations who are the most marginalised, and who remain most vulnerable to prosecution, despite advances in HIV science that are being used to challenge and modernise these laws.
Writing in the Journal of the International AIDS Society, the authors – who include HJN’s Executive Director, Edwin J Bernard; HJN’s Supervisory Board member, Michaela Clayton; and HJN’s Global Advisory Panel member, Edwin Cameron, along with Chris Beyrer, Desmond M. Tutu Professor of Public Health and Human Rights at the Johns Hopkins Bloomberg School of Public Health and GNP+’s Alexandra Volgina – note that despite many advances in the science of HIV there remains one area that is still an “all too common a threat to the lives and wellbeing of people living with HIV, as well as to the goal of ending the epidemic” – HIV criminalisation.
HIV criminalisation describes the unjust application of criminal and similar laws to people living with HIV ostensibly based on their HIV status, either via HIV‐specific criminal statutes or general criminal or other laws.
Citing data collated from HJN’s global case monitoring which suggests that HIV criminalisation intersects with “discrimination or criminalization on the basis of ethnicity, sex, gender identity, immigration status, sex work, sexuality and/or substance use,” they note that HIV criminalisation can be seen as a “surrogate marker for state‐sponsored stigma and discrimination against marginalized groups of people at higher risk of HIV.”
The editorial also addresses public health and healthcare workers who are often viewed as an extension of the criminal justice system by marginalised populations. “We are also seeing a frightening trend of prosecutions being initiated by those working in healthcare or public health without specific complaints. In some cases, police were notified of a person’s HIV diagnosis by health authorities, which then became a prompt to investigate the person’s relationship with their partner.”
“It is important that we all understand how to ensure justice for all people living with HIV, not just those who have access to treatment and are fortunate enough to be undetectable,” they conclude, “so that we can finally end these outrageously unjust laws, policies and practices against people living with HIV in all of their diversity.”
WATCH! From Moment to Movement: HIV Justice Live! Ep 3 – Oslo Declaration 9th Anniversary
From Moment to Movement: HIV Justice Live! celebrates the Oslo Declaration on HIV Criminalisation
The 3rd episode of HIV Justice Live! aired on Wednesday, February 17, to celebrate nine years since the publication of the historic Oslo Declaration on HIV Criminalisation. Hosted by HIV Justice Network’s Edwin J Bernard, the show featured some of the advocates who were behind the Oslo Declaration.
Kim Fangen, co-organiser of the side-meeting that finalised the Oslo Declaration, and who was the only person openly living with HIV on the Norwegian Law Commission, revealed that the Declaration was initially conceived as an advocacy tool to influence policy discussions in Norway as well as neighbouring Nordic countries.
Patrick Eba, now UNAIDS Country Director in the Central African Republic, explained that the reason the meeting took place in Oslo was because the Norwegian Government had supported UNAIDS to produce detailed guidance on how countries should deal with the overly broad use of the criminal law to HIV non-disclosure, exposure and transmission, by examining scientific, medical and legal issues.
Former ARASA ED, Michaela Clayton, now a member of HJN’s Supervisory Board, said the Oslo Declaration was the first time there was a coming together of activists from both the global north and south around HIV criminalisation. She noted that although there had been some work done regionally and in-country, this was the first global solidarity statement around HIV criminalisation.
Ralf Jürgens, now Senior Coordinator of Human Rights at The Global Fund, who attended the Oslo meeting in an advisory capacity, spoke about his relief and delight that the work that he and others had done as part of the ‘first-wave’ of advocacy against HIV criminalisation was now being undertaken by the HIV Justice Network. Jürgens currently oversees the innovative Global Fund initiative, Breaking Down Barriers, which supports 20 countries to remove human rights-related barriers to health services for HIV, TB malaria, and COVID-19. He said the Global Fund has invested resources to fight laws and policies and discrimination overall and ensure access to justice. He added that the HIV Justice Worldwide movement now plays an “incredibly important” part in this work by providing global leadership and a wide range of advocacy resources.
There was a surprise appearance by Susan Timberlake, who was UNAIDS’ Senior Human Rights Advisor when the Oslo meetings took place. She recognised the Oslo Declaration as the moment that the global movement around HIV criminalisation began. Susan recalled the main meeting fell on Valentine’s Day and participants made posters with “make love, not criminal laws” messaging.
Our regular Mind the Gap segment featured Ellie Ballan, a member of our Global Advisory Panel, who is based in Lebanon. He was interviewed by Julian Hows, HJN’s Partnerships and Governance Co-ordinator.
The Oslo Declaration, has so far, garnered over 1750 signatories from more than 115 countries and been translated into nine different languages, the most recent being Latvian and Turkish. It was also the template for the Mexican Declaration in 2017. Pozitif Dayanışma, an HIV organisation based in Turkey recently translated the Declaration into Turkish, as well as producing an accompanying info-graphic and social media pack.
Further, the Oslo Declaration has been referred to as key guidance on HIV criminalisation from global organisations such as UNAIDS, Amnesty International, and PEPFAR/USAID, cited in several peer-reviewed journals and used as a strategic planning and advocacy tool all over the world. The Declaration has also been featured in high-profile media, such as the New York Times, the Huffington Post, and POZ magazine.
Australia: New South Wales mandatory testing bill is unnecessary and could be counterproductive
Mandatory disease testing bill ‘could put officers at risk’
NSW Health says a proposed law enabling authorities to force people to undergo testing for bloodborne diseases could actually put frontline workers at greater risk.
The department’s evidence to a parliamentary committee came as a senior NSW police official said it’s “not unusual” for officers to get pelted with faeces mixed with blood.
Getting bitten, spat on, or splashed with blood are some of the unfortunate realities faced on the job by emergency and prison workers, and come with the additional fear of getting infected with bloodborne diseases.
But the risk of infection from such incidents is very low, and drawing blood samples from people against their will could make them less likely to trust health workers to perform voluntary tests, a top NSW Health official said.
Such an increase in mistrust could make it harder for health workers to combat the spread of the diseases, including among prisoners where the prevalence of hepatitis C is up to 20 per cent higher than in the general community, the committee heard.
“The importance of reducing any stigma and discrimination, and improving the quality and accuracy of information about bloodborne viruses is paramount to engaging people in treatment,” said Michelle Cretikos, executive director with NSW Health‘s population and public health division.
“If people are discouraged from accessing treatment, then in fact the risk may increase, both to the people in the community as well as the workers that are looking after them.
“It‘s likely to reduce people’s trust in the health services … and may reduce access to treatment and access to care.”
Since 1994, there have been zero cases of NSW healthcare workers getting infected with HIV after an exposure in the workplace, Dr Cretikos said, pointing to an NSW Health policy directive.
That same directive included a survey of international studies, including an Australian one, all of which failed to turn up a single case of HIV transmission to healthcare workers after exposure to the virus.
“There have been zero, zero, zero, zero, zero, zero cases in all of those studies … And that’s correct over many years, across many countries,” Dr Cretikos said.
Even when the exposure was in the form of a needle puncture, the transmission risk was calculated at 0.3 per cent.
One Brazilian study conducted between 1997 and 2009 that looked at 80 cases of healthcare workers getting exposed to HIV via needle prick injuries found that none of the workers were infected.
For hepatitis C exposure, the rate of transmission was slightly higher, with a range of nine international studies showing a rate between zero and 2.3 per cent.
That included an Australian study which showed no instances of transmission among 64 incidents of puncture injuries caused by large needles.
A top corrective services official said similar data was difficult to collect for prison staff, because workers were not mandated to let their employers know whether they had a disease or not.
But the fact that there is a risk means there is a need for greater protection, said Gayle Robson, chief of staff to the commissioner of Corrective Services NSW.
“It is (…) sufficient, there is simply a risk of our staff contracting bloodborne viruses,” Ms Robson said.
There was no risk of bloodborne virus infection from many other body fluids such as urine, spit or faeces, or when the skin wasn’t breached, the NSW Health document said.
NSW police deputy commissioner for corporate services Malcolm Lanyon told the committee that out of some 2,500 assaults on police last financial year, 490 involved exposure to bodily fluids, including 69 bites and 29 needlestick injuries.
He said being able to force people to undergo disease testing would significantly reduce the anxiety officers feel when they’ve been exposed to bodily fluids.
“Waiting periods associated with self-testing of the police officer can lead to months of uncertainty, which can be enormously stressful and have lasting psychological impacts on officers and their family,” Commissioner Lanyon said.
And while non-blood body fluids might not pose a disease risk on their own, officers were often exposed to a mix of substances that included blood, he said.
“There are a number of disgusting and degrading acts that happen often when someone is in custody in a cell … It’s not unusual for them to deliberately defecate in there, it’s not unusual for people to then self-harm in that cell, get blood mixed with faeces, and throw that at police officers. That’s not an unusual scenario in custody.”
Corrective Services director Craig Smith similarly said that corrective officers suffer a blow to their mental health when faced with uncertainty over whether they could have been infected.
“I’ve seen grown men cry,” Mr Smith said.
“I agree that the risks are low, (but) it‘s that ‘maybe’.”
Year in review: Celebrating successes, highlighting the many challenges ahead
This past year has shown us what happens when one pandemic – HIV – is overshadowed by another pandemic, COVID-19. Despite the many lessons learned from our collective advocacy against HIV criminalisation that we and our HIV JUSTICE WORLDWIDE partners highlighted in March, these lessons were mostly ignored by policymakers around the world.
The result was a series of knee-jerk legal, policy and police responses leading to the overzealous policing of people living with HIV and other key and inadequately served populations already subject to existing inequalities in law and policy, which we have been highlighting in our HIV Justice Weekly newsletter since March.
This latest pandemic overshadowed, and in some cases undermined, the work we and others have been doing to ensure a fair, just, rational and evidence-based response towards people living with HIV by the criminal justice system.
2020 also saw Poland passing a new law against COVID-19 that also increased the criminal penalty for HIV exposure, and number of disappointing HIV criminalisation higher court appeals in the US (Ohio), and Canada (Ontario and Alberta) that appeared to ignore science over stigma.
And yet, despite the many difficulties of 2020, the movement to end unjust HIV criminalisation has continued to gain momentum.
There is still so much more to do, however. Despite these successes, as well as the many milestones the HIV JUSTICE WORLDWIDE movement has achieved since its launch in 2016, we will not rest until everyone living with HIV in all their diversity is treated equally, fairly and justly by all actors of the criminal justice system.
UK: Police Federation working with the National AIDS Trust to tackle HIV stigma and misinformation
The Federation is working with the National AIDS Trust to tackle the stigma of HIV and provide reassurance for colleagues around its transmission.
Over the decades, many officers have been spat at or bitten by individuals who ‘weaponise’ the virus by claiming to be infected. But the chances of acquiring HIV through spit or a bite are close to zero, and no police officer has ever acquired it in this way.
There are only three ways a person can be infected – needle sharing, sexual intercourse and breastfeeding.
PFEW National Board member Simon Kempton, who has led on the issue of communicable diseases, said: “The act of spitting at a police officer is vile, is disgusting and particularly during a global pandemic carries risks of transmitting other diseases. But we know from decades of research that it’s impossible to transmit HIV by that method, and people who threaten us with that only increase that feeling of fear and stigma.
“The Federation is keen to help colleagues understand the true risks of transmission, to help them deal with the fear factor that’s been built in unnecessarily. Knowledge IS power and helping officers to understand how negligible the risks are is important to their mental health after being assaulted.”
HIV if left untreated, attacks the immune system. However, if caught early and treated, it will not lead to AIDS which is the advanced stage. AIDS is now very uncommon in the UK thanks to effective treatment and people living with HIV can live full and productive lives with normal life expectancy.
Since HIV is now classed as a disability and a protected characteristic, it is not appropriate to record HIV status as a warning marker on police databases, except in situations like Custody where treatments might need to be administered.
DC Tracy O’Hara QPM of Merseyside Police explained: “These markers should only be on a custody record health assessment and even then, only available to those who need to know this information. So, if someone says, ‘I live with this condition and I need my medicine’ that should be on the record, but HIV status is not something the police service should be disclosing nor holding as warning markers or flags.
“It is important to note that we have colleagues living with HIV. How must they feel when we add to stigma or we store this information in such a negative way? They are never going to feel comfortable sharing their status to ensure their health is looked after. So this is not simply about our communities it is about our colleagues as well.”
A series of articles and editorials in the October 2020 issue of the American Journal of Bioethics published last Friday examine a growing concern amongst community leaders of people living with HIV and our scholarly allies: the use of blood taken from people living with HIV during routine testing prior to starting or changing antiretroviral therapy in surveillance databases, without our permisssion, for public health purposes.
This is already taking place across the United States and in some Canadian provinces, and is currently being considered elsewhere in the world.
The rollout of so-called ‘molecular HIV surveillance’ to identify ‘clusters’ of transmissions to attempt to further improve public health responses to HIV is a growing source of anxiety and concern for people living with HIV in the US and Canada, especially for people who are already marginalised and criminalised in other ways, because they can’t be certain that this data won’t be shared with law enforcement or immigration authorities, which can lead to prosecution and/or deportation.
Coming to Facebook Live on 30th September – HIV Justice Live! Whose Blood is it, Anyway? Like or follow us on Facebook to watch and participate in the first of our new interactive webshows, which will focus on molecular HIV surveillance.
“HIV data justice draws on the collective resources of the HIV/AIDS movement to build new alliances aimed at providing affected individuals and communities with greater control over how their data are utilized in the healthcare system, with the paired aim of providing them with greater access to better services on terms of their own choosing.”
Molldrem and Smith
In the editorial, we welcome Molldrem and Smith’s critique of the controversial rollout of molecular HIV surveillance (MHS) in the United States, which explores three intersecting concerns:
(1) the non-consensual re-purposing of personal health information and biomaterial for public health surveillance;
(2) the use of molecular HIV surveillance data in larger databases to find ‘clusters’ of infections and to make determinations about transmission directionality, and the criminalising implications that follow such determinations; and
(3) the way MHS amplifies the targeting and stigmatisation of already oppressed and marginalized communities.
The editorial questions the rationale behind the use of MHS as one of four pillars of the US Centres for Disease Control (CDC) End The Epidemic (ETE) Plan and calls for the abolition of molecular HIV surveillance in the United States as it is currently being rolled out by the CDC because it blurs the boundaries between consent and criminalisation.
Instead, we envision a future of new participatory and intersectional racial and viral justice possibilities, one which ensures the lives, voices, self-determination, and autonomy of people living with HIV are central to HIV research and public health practice.
You can select your preferred language from the 'Select Language' menu at the top of the page.
Continue
We use cookies to ensure that we give you the best experience on our website. By continuing to use our site, you are agreeing to our use of cookies. You can change your cookie settings at any time if you want. Find out more in our Privacy & Cookie Policy.