Honouring the courage of transgender people globally, especially transgender people living with HIV
Today is International Transgender Day of Visibility, held annually on 31st March to celebrate transgender people globally and honour their courage and visibility to live openly and authentically.
This year’s 14th annual celebration is a day to also raise awareness around the stigma, discrimination and criminalisation that transgender people face.
According to the Human Dignity Trust, 14 countries currently criminalise the gender identity and/or expression of transgender people, using so-called ‘cross-dressing’, ‘impersonation’ and ‘disguise’ laws. In many more countries transgender people are targeted by a range of laws that criminalise same-sex activity and vagrancy, hooliganism and public order offences.
Transgender people living with HIV can be further criminalised based on their HIV-positive status, although we know that there are still too many invisibilities around the impact of HIV criminalisation on transgender people.
Cecilia Chung, Senior Director of Strategic Initiatives and Evaluation of the Transgender Law Center, who is also a member of our Global Advisory Panel told our 2020 Beyond Blame webinar that there are not enough data on the impact of HIV criminalisation laws on transgender people. She said such data are not “uniformly collected across the world… The numbers still remain invisible even though we know for sure there are [HIV criminalisation] cases.”
HJN honours the courage of transgender people – especially transgender people living with HIV – to live openly and authentically. We also call for more visibility for transgender people in data collection, as well as reforms of all criminal laws and their enforcement that disproportionately target transgender people.
The 24th international AIDS conference (AIDS 2022) held in Montreal and virtually between 29 July and 2 August integrated HIV criminalisation throughout multiple sessions – both in the main conference and during pre-conferences, satellites and in the Global Village.
Australian activist, lawyer, Track F rapporteur – and HJN Supervisory Board member – Paul Kidd has provided a thorough overview of many of these sessions in this Twitter thread, which can also be read as a single blog entry here.
Two major campaigns were launched at the conference – one global, and one focused on Canada.
GNP+ and HJN joined with networks representing young people, women, the LGBTI+ community, sex workers and people who use drugs to launch the “Not A Criminal” Campaign to decriminalise HIV non-disclosure, exposure and transmission; same-sex relationships; sex work and drug use.
As part of the “Not A Criminal” Campaign, we are demanding countries remove bad laws and replace them with evidence-based legislation to protect our communities from criminalisation, discrimination and gender-based violence, and support the creation of independent human rights institutions. Additionally, the campaign calls on United Nations agencies and donors to develop strong, coordinated, and high-profile mechanisms to monitor progress on these member states’ commitments.
“Far from being a legitimate public health tool, criminalisation of our behaviours, choices and identities is about the enforcement of an oppressive morality through policing our bodily autonomy,” HIV Justice Network’s Executive Director Edwin J Bernard said in a press release announcing the campaign. “This punishment of our vulnerability also means we won’t be able to end the HIV epidemic by 2030.”
The Canadian Coalition to Reform HIV Criminalization (CCRHC) made the most of the spotlight on Canada during the conference and launched its second Community Consensus Statement. This Statement calls on the Canadian government to change the Criminal Code to limit HIV criminalisation only to very rare cases of intentional transmission using appropriate existing criminal statutes. Canada’s Justice Minister, David Lametti has since announced plans to launch a consultation this October on the criminal legal system’s overly draconian response to HIV non-disclosure.
However, the biggest – and most welcome – surprise of the conference was the recipient of the Elizabeth Taylor Legacy Award which was presented during Saturday’s prime session on HIV and Human Rights. Previous recipients have included Nancy Pelosi, Sharon Stone, Whoopi Goldberg, Michael Jackson and Elton John.
This year’s Elizabeth Taylor Legacy Award was presented posthumously to the late Rosemary Namubiru – recognising her extraordinary contribution to raising awareness of the injustice of HIV criminalisation.
Lillian Mworeko of the International Community of Women Living with HIV – East Africa (ICW-EA) received the award on behalf of Rosemary’s family. Rosemary’s daughter had planned to be there, but – like many Africans – was denied a visa.
Our own @lmworeko received the Posthumous Elizabeth Taylor legacy award on behalf of Rosemary Namubiru & her family in 🇺🇬. Rosemary, a dedicated nurse, was imprisoned for her HIV status. @richardlusimbo called upon everyone to confront HIV criminalisation #AIDS2022pic.twitter.com/3sBB9mvPRA
UGANET joins the family of the late Rosemary Namubiru and the HIV Community at large to celebrate the posthumous Elizabeth Taylor AIDS Foundation Award awarded to her in Montreal, Canada, on 30th July 2022.
Today we are delighted to share with the world a new short film, Mwayi’s Story, produced by the HIV Justice Network on behalf of HIV JUSTICE WORLDWIDE.
We wanted to produce a film that was authentic to the lived experience of an HIV criminalisation survivor but without making her go through the trauma of having to relive the experience by telling her story again.
HJN’s video, visuals and webshows consultant, Nicholas Feustel, who produced and directed the film, said: “Since this story is primarily about mothers and children, we decided to produce the film in the style of an illustrated children’s storybook. We searched for a female illustrator working in sub-Saharan Africa and found the wonderful Phathu Nembilwi of Phathu Designs.
“For our narrator, we found Upile Chisala, a storyteller from Malawi known for her short and powerful poems.”
The script by HJN’s Senior Policy Analyst, Alison Symington, was written in consultation with our Supervisory Board member, Sarai Chisala-Tempelhoff, a Malawian human rights lawyer and legal researcher with over 15 years of experience in women’s access to justice.
We also worked with our HIV JUSTICE WORLDWIDE partners, Southern Africa Litigation Centre (SALC) and AIDS and Rights Alliance for Southern Africa (ARASA), to ensure that the film was relevant to their ongoing advocacy in the region. In fact, Mwayi’s Story had its world premiere last week on Zambia’s Diamond TV, in anticipation of a verdict in a similar breastfeeding case.
The film will be shown in a number of forums over the next few months, including at AIDS 2022. It will soon be subtitled in French, Russian and Spanish, and we are also looking for partners to translate additional subtitles if they think the film can be useful in their own advocacy. If you’re interested you can get in touch with us at breastfeeding@hivjustice.net. We will send you the English subtitle file for translation. After you return the file to us, we will upload it to YouTube.
Mwayi’s Story is part of our ongoing work to end the criminalisation of women living with HIV for breastfeeding and comfort nursing, including our Breastfeeding Defence Toolkit. It is our goal to collaborate with advocates, researchers, service providers, organisations and community members around the world to raise awareness and prevent further unjust prosecutions against women living with HIV who breastfeed or comfort nurse. We are grateful to both the Elizabeth Taylor AIDS Foundation and the Robert Carr Fund for their financial support for this work, and this film.
New report shows how women living with HIV are leading the response against HIV criminalisation in the EECA region
The report illustrates how HIV criminalisation and gender inequality are intimately and inextricably linked. By highlighting prosecution data from Belarus, Kazakhstan, Russia and Ukraine disaggregated by sex, the report shows how the burden of HIV criminalisation is falling upon women.
The report also includes some heart-breaking personal stories including that of a woman in Russia who was prosecuted for breastfeeding her baby, as well as several women in Russia blackmailed by former partners who threatened to report them for alleged HIV exposure as a way to control, coerce, or abuse them.
The evidence provided in the report clearly demonstrates that HIV criminalisation not only fails to protect women from HIV, but worsens their status in society, making them even more susceptible to violence and structural inequalities due to the way their HIV-positive status is framed by the criminal law.
The report goes on to explore how women living with HIV in the region are vulnerable to a range of economic consequences including loss of property, as well as ostracism and discrimination in their communities, including being separated from their children, because:
Women living with HIV’s reproductive and maternal choices are controlled by, and can be abused by, the state.
Women living with HIV in partnerships with HIV-negative men can be threatened with prosecution, or be prosecuted, even if there has been prior disclosure and consent to the ‘risk’ and even when condoms were used or the woman had an undetectable viral load.
Confidential medical information can be illegally shared with law enforcement agencies.
The report also shows a direct connection between HIV criminalisation and other forms of criminalisation – notably the use and possession of drugs, and of sex work – that exacerbate the burden of discrimination, the violation of rights, and violence experienced by women living with HIV in the region.
Despite the difficult picture painted, the report provides hope, however.
It is the mobilisation of the women’s community and the meaningful participation of HIV-positive women and their allies in advocacy for law reform, rights protections – and in the preparation of alternative reports to UN Committees such as the Committee on the Elimination of Discrimination against Women (CEDAW) – that are making a real difference in the fight against HIV criminalisation in the region.
Rosemary was a dedicated nurse as well as a mother and grandmother – and a courageous HIV criminalisation survivor. In 2016, at our Beyond Blame pre-conference to AIDS 2016 in Durban, South Africa, she spoke with great dignity about her horribly unjust experiences at the hands of the criminal legal system and media.
In January 2014, Rosemary was wrongfully accused of intentionally exposing a child to HIV while administering an injection. The child did not acquire HIV. However, the accusations created a media frenzy at a time when Uganda was discussing whether to enact the HIV Prevention and Control Actthat, amongst a number of problematic provisions, allows for stringent punishments for the vague ‘crimes’ of attempted and intentional HIV transmission.
The inflammatory media coverage, which included showing her arrest live on television, meant that she was found guilty in the court of public opinion long before her trial, singled out and vilified in the press because of her HIV-positive status.
Originally charged with attempted murder, she was eventually convicted of criminal negligence. However, on appeal, the judge found that her initial three-year sentence was excessive and ordered her release after she served 10 months in prison.
Rosemary was supported at the time by several advocacy and human rights organisations including the International Community of Women Living with HIV, Eastern Africa (ICWEA), Uganda Network on Law, Ethics and HIV/AIDS (UGANET), The National Forum of People Living with HIV in Uganda (NAFOPHANU) and AIDS-Free World.
Following her release, in a meeting arranged by AIDS-Free World, media editors finally heard her side of the story and apologised to her. ICWEA continued to support Rosemary following her release, and remained in touch until her death.
This experience has totally changed my life. My self-esteem is gone and this has tarnished more than 30 years in the nursing profession, which I loved so much. I still struggle to overcome that fateful day when I woke up in the morning to go and save lives, only to be beaten down by the world.
I now know first-hand that stigma, especially among healthcare workers, is real. I’ve lost everything. I had a job, I was the breadwinner for my family, and I belonged to a community. I would give anything to be able to go back to my old self. I still need support to regain my strength, start generating an income again, and feed my family.
It is my hope that by telling my story it will show the real struggle we face against stigma and criminalisation. I saw it all, I faced it all, and I don’t want anybody else to go through it. Together, we need to fight for others who are experiencing these acts of injustice.
UPDATE JULY 2022
In July 2022, Rosemary was posthumously awarded the Elizabeth Taylor Legacy Award at AIDS 2022 in Montreal.
Previous recipients include Sharon Stone, Whoopi Goldberg and Elton John.
The award recognised her extraordinary contribution to raising awareness of the injustice of HIV criminalisation.
Lillian Mworeko of the International Community of Women Living with HIV – East Africa (ICW-EA) received the award on behalf of Rosemary’s family.
Our own @lmworeko received the Posthumous Elizabeth Taylor legacy award on behalf of Rosemary Namubiru & her family in 🇺🇬. Rosemary, a dedicated nurse, was imprisoned for her HIV status. @richardlusimbo called upon everyone to confront HIV criminalisation #AIDS2022pic.twitter.com/3sBB9mvPRA
UGANET joins the family of the late Rosemary Namubiru and the HIV Community at large to celebrate the posthumous Elizabeth Taylor AIDS Foundation Award awarded to her in Montreal, Canada, on 30th July 2022.
Tiffany Moore had a panic attack at a Tennessee playground. That’s how her 2021 ended.
All she’d wanted was to give her 8-year-old daughter the gentle childhood she’d never had. By age 10, Moore had for years been strapped down repeatedly in mental health wards and “pumped full of drugs” in different hospitals. That was in addition to the abuse she’d experienced at home. Half a decade later, she would be on the streets, surviving through work with sex traffickers and pimps. At age 10, she says, she didn’t expect to see adulthood. Now, as a mother, she was determined her daughter would grow up enjoying her childhood experiences, including afternoons on swings and slides with her mommy.
But until December 2021, when a change in Tennessee law that she fought for went into effect, Moore was legally forbidden from visiting a playground. That’s because at 21, she was convicted of aggravated prostitution—the aggravation being that she’d acquired HIV during a rape. And even though she did not transmit HIV to anyone, Moore spent 20 years on Tennessee’s sex offender registry as a result of her status.
Within weeks of her removal from the registry, Moore was at a playground surrounded by children, and every fiber in her body told her to flee, that she was one call to the police away from being separated from her daughter.
“They’ve instilled for 20 years that you’re a danger to children and your child. You can’t go here; you can’t go there. You can’t be here; you can’t be there,” she says. “I just know—I know I have a lot of pieces to pick up.”
She’s not alone. Though the public face of HIV criminalization laws has been primarily gay men—particularly gay Black men—recent data show that such legislation also targets Black women.
In particular, research conducted by the Williams Institute at the University of California at Los Angeles has found that in California, for instance, Black women make up 3% of the population and 4% of people living with HIV but 22% of people prosecuted under that state’s old HIV criminalization law.
In Georgia, Black women make up 17% of the population and 18% of those living with HIV but fully half of people prosecuted under that state’s HIV criminalization laws. In Kentucky, which has a law similar to Tennessee’s, 32 people have been arrested on HIV criminalization charges. All but one of those charges was associated with sex work. In that state, those arrested have mostly been white women. According to an article in a Tennessee newspaper, by 2009, 38 people besides Moore had been arrested under the aggravated prostitution charge.
“The image we have around HIV criminalization laws maybe is of a gay cisgender man who doesn’t disclose his status to a sex partner,” says Nathan Cisneros, MS, the Williams Institute’s HIV criminalization analyst and the coauthor of the Kentucky study as well as a forthcoming report on Tennessee’s laws.
“What we find in states that have prostitution-specific HIV laws, though, is that sex work ends up taking on a substantial minority, sometimes a majority and sometimes the overwhelming majority of enforcement actions. And those primarily affect women,” he says.
Because arrest records reflect someone’s assigned gender at birth and not their preferred gender, it’s unclear how many of those arrested are women of transgender experience living with HIV, but other data suggest that this group is overrepresented among sex workers nationwide.
Yet women with HIV aren’t just the target of these laws—they are also fighting them, forming coalitions, writing legislation and, like Moore, testifying about the science and impact of the laws to effect change.
Today, 30 states have statutes specifically prosecuting people living with HIV for real or imagined crimes related to HIV transmission or exposure, according to The Center for HIV Law and Policy.
The list of potential crimes reads like an HIV stigma fever dream. In some instances, people with HIV can be arrested for allegedly not telling a partner they are living with the virus—even if they are taking HIV medications and are undetectable, which eliminates the risk of transmitting it to a partner.
They can be prosecuted even if they did tell the partner they were living with HIV but their partner tells the police that they didn’t. In other instances, people living with HIV can be arrested for exposing others to bodily fluids, including via spitting and biting, acts that don’t transmit HIV. Yet other laws prosecute syringe sharing among people living with HIV who inject drugs, and still more criminalize even semen donation by those who are HIV positive and want to become parents.
In addition, nine states have so-called sentence enhancements that can take a preexisting charge unrelated to HIV and increase prison time and penalties for people living with the virus. Six states may require people living with HIV who are found guilty to register as sex offenders.
The states that specifically increase the severity of penalties for people involved in sex work primarily impact women living with HIV. In Tennessee, where Moore lives and served time, a sex work charge alone is a misdemeanor, punishable by a fine. But add in the HIV charge and suddenly a woman is facing a felony, punishable by years in prison. That conviction also requires registration as a sex offender, with the heightened punishment of being classified as a violent offender.
“It makes it difficult to get housing and stable employment, to receive certain benefits, to vote in elections,” Cisneros says. “And of course, if you have children, it creates all these other terrible complications. You can’t pick your child up from school. You can’t visit them at the playground. You can’t have your children’s friends over for a sleepover.”
From the beginning, Moore’s experience of living with hiv was intertwined with incarceration. When she was arrested for sex work in March 2002, the state of Tennessee also required her to get an HIV test. That’s when she found out she was living with the virus.
But she wasn’t allowed a private moment to process it. Instead, when court staff read out the charges at her arraignment, “my status was read out loud in court,” she remembers. For her, she says, that was the “initial attack” in a yearslong journey through the court system.
She wasn’t offered care or services. She simply left jail and went back to her former life. She evaded the public health workers who were circulating her name and photo among the traffickers who could use it to hurt her. She was 20, not even legally able to drink. To cope, she’d been cutting herself for years. When that failed to stop the terror and flashbacks, she turned to crack.
“That was my Prozac,” she says. “My entire left wrist is cut up from my coping skills. [Using drugs] was the way to not cut myself. That was the only way I knew to keep myself safe.”
Now that she knew her HIV status, future arrests carried with them the extra weight of the criminalization statute. By August 2002, she’d been arrested again and could either stand trial, which could result in a 15-year prison term, or she could plead guilty to the charges and accept a four-year sentence with no possibility of parole and be added to the sex offender registry as a violent offender. No one had acquired HIV from her. She hadn’t even been engaged in sex work when the arrest happened. She’d just been loitering in a prostitution zone while living with HIV.
That began what would eventually total eight and a half years behind bars, off and on—always being released between 11 p.m. and 2 a.m., always finding johns waiting for her and always finding that drug treatment centers couldn’t take her because of her HIV diagnosis or her status as a registered sex offender. Halfway houses were out of the question—the sex offender registry again. It was maddening, Moore says now. She wanted to get off the streets, but the criminal code kept her stuck.
One thing did change during this time. She started on HIV meds in prison, at first on drugs that made her sick every day. About three years into her first term, she had an undetectable viral load, which means she couldn’t transmit the virus. But that didn’t stop the arrests from coming.
“I was always arrested before the medication ran out,” she says, so her treatment wasn’t interrupted.
In the Kentucky report from the Williams Institute, Cisneros and colleagues found that most of the arrests were made on the streets or in parking garages. At least 15% of arrests were “almost certainly for conduct that did not involve sex work. Indeed, arrests for allegations of sex work do not need to include actual sex acts.”
In 2011, Moore left prison for the last time. She finally found a treatment center that would accept her despite her status on the sex offender registry. She quit drugs. She started working with an HIV service organization and for the first time began addressing her posttraumatic stress disorder. Importantly, she finally connected with others living with HIV through the Sero Project, a group of people with the virus who are working to change criminalization laws.
And, almost as quickly, she started working to modernize Tennessee’s HIV laws. By 2015, she was also a new mom. What’s more, for the first time, she had her own apartment, a car and a job.
“I started to realize,” Moore says, “that what was done to me wasn’t right.”
Again, moore wasn’t alone. women and nonbinary people living with HIV have been working along with gay men to guide the decades-long effort to reform HIV criminalization laws.
Whether it’s Tami Haught, who was key to getting Iowa to remove people living with HIV from the sex offender registry in 2014, or Barb Cardell, who advocated successfully in Colorado for the elimination of mandatory HIV testing for people arrested for sex work and the removal of felony charges from someone living with HIV convicted of sex work, or Naina Khanna and other members of Positive Women’s Network–USA, who worked to reduce sex work charges for women with HIV from felonies to misdemeanors, women living with HIV have been guiding the movement against HIV criminalization for years.
And that doesn’t even include advocates living in states that have yet to reform their laws, like Indiana, Georgia and Ohio.
So in 2015, when Moore testified before the Tennessee Statehouse to advocate for people placed on the sex offender registry to be able to have themselves removed if they had been sex trafficked, raped or abused, she was part of a bigger sisterhood. But it came at a price. She went back to her old coping mechanism. She relapsed. It was the first time, she says, that she knew what it was like to lose everything because “before, I had nothing.”
In the last seven years, though, Moore has held on to her recovery with both hands.
“I grew up,” she says. “It was like, literally, wisdom overnight.”
Now, she’s stepping into advocacy again. She is part of a complaint filed by The Center for HIV Law and Policy asking the Department of Justice to investigate HIV criminal statutes in Tennessee and Ohio. And it looks like the tide is turning.
In 2016, the Association of Nurses in AIDS Care released the first clinical guidelines on addressing HIV criminalization, and the American Psychological Association officially came out against HIV criminalization laws. This was followed by a consensus statement issued in 2018 by the world’s premier HIV scientists and clinicians arguing that laws should be revised to reflect the actual science of HIV transmission.
The following year, the American Medical Association came out against the laws. Now, the Centers for Disease Control and Prevention’s website has a page dedicated to how HIV criminalization laws are inconsistent with the national effort to reduce new HIV transmissions by 90% by 2030.
For Moore, being removed from the sex offender registry at the end of 2021 was bittersweet. The aftereffects linger, she says, and she still thinks about how Tennessee’s law might be different had she been able to tolerate “the uncomfortable second” that comes with the overwhelming urge to hide in just one more inhalation on a crack pipe.
As written, the law requires people seeking removal from the list to prove that they were abused, raped or otherwise sex trafficked in order to gain their freedom. Courts can require trials that force women to come up with proof of the abuse.
Now, Moore says she’s on a new healing journey, with the registry behind her. She will continue to pick through the traumatic effects of surviving her childhood and living with the stigma of the registry. Still, when she sees her daughter playing in her own room, surrounded by all the things she didn’t have growing up, in an apartment Moore pays for with a job she selected, with a car she owns parked outside, she says a sense of peace and happiness comes over her.
“I just want her to be a kid,” she says. “There’s so much time for her heart to be broken by the world we live in right now. I just want her to play with slime and dolls.”
Tajikistan: Imprisoned for living with HIV – A woman’s testimony
“An HIV diagnosis should not be a guilty verdict—it’s just a diagnosis”
Nargis was born in Dushanbe, Tajikistan, into a large family. Life was not easy, and she was sent to a boarding school for low-income families. Her favourite subject at school was physical education, excelling at basketball and swimming. She hoped that after graduating from school in 1991 with a diploma in physical education she would continue her studies at a technical school.
However, because of unrest in the country, she couldn’t carry on with her schooling. “I cried for six months, I really wanted to continue my studies, but instead of going to a technical school, my parents married me off. I was not yet 16 years old then,” said Nargis. When she was 17 years old, she gave birth to a son; five years later, while pregnant with her second child, she learned that her husband was involved in drug trafficking, and he was sent to prison.
From that time on, Nargis had to provide for herself and her family on her own. She got a job in a casino. The earnings were good, but it was there that she started taking drugs. “I was a shy girl, so to make me feel relaxed, I used drugs. From there, I became a drug addict. I didn’t even notice how it happened,” she recalled.
She was eventually fired from her job because of her drug-taking and was forced to look for other ways to survive.
Nargis injected drugs for 14 years, but she started on opioid substitution therapy when it was made available in the country. “While I was on methadone, I was hired as a peer counsellor. I worked with drug users, with people living with HIV. I worked as a consultant in several HIV prevention projects,” said Nargis.
Nargis remained on methadone until May 2021. “Last year, I had to stop methadone because I was sent to prison and there was no methadone in prison. It was very hard, I was in the prison hospital for several months, but as a result I got off methadone and, so far, I am holding on.”
Nargis was imprisoned under Article 125 of the Criminal Code of Tajikistan, under which it is a criminal offence to infect someone with HIV or to put them at risk of HIV infection. Based on this article, law enforcement agencies initiate criminal cases against people living with HIV just on the basis of the potential threat of HIV transmission or simply just based on their HIV-positive status.
“I have been taking antiretroviral therapy since 2013. I have never interrupted it. I have an undetectable viral load. No one wrote a statement against me. I did not infect anyone. The accusation was made on the basis of a note from a man I knew, because we were dating,” Nargis said.
The legislation does not take into account the informed consent of the other sexual partner, regardless of whether there was a risk of HIV infection, or whether the person living with HIV takes precautions against HIV transmission. In addition, the legislation does not define how someone living with HIV should declare their HIV status. In effect, all people living with HIV who have sex can be held criminally liable.
Nargis explained her shame, “Law enforcement agencies called everyone, doctors, my colleagues, relatives, and told them about my HIV diagnosis, asked what kind of relationship we were in, dishonoured me.”
“Article 162 of the Health Code gives doctors the right to disclose the status of HIV-infected patients at the request of the investigating authorities, and does not contain any justification for this. Some criminal cases under part 1 of Article 125 were initiated after the HIV clinic disclosed information about HIV to law enforcement agencies. During the investigation and trial, the defendants’ right to confidentiality regarding their HIV status is not ensured, since investigators, officials, court clerks and judges can request medical information in accordance with the provisions of the Health Code without any specific conditions,” said Larisa Aleksandrova, a lawyer.
Nargis is now free, but she said that she was just lucky. “I was released under an amnesty in connection with the 30th anniversary of the republic.”
She is out of prison, but there are still dozens of other people convicted under Article 125. Now that everyone knows that she is living with HIV, Nargis is ready to fearlessly fight for the right to live, work and love, despite her HIV status.
Nargis continues to work as a volunteer peer consultant on HIV prevention. She has many plans, but the main goal that she is striving for is the revision of articles criminalizing HIV in Tajikistan.
“I always say that there should be more information about HIV, about people living with HIV, so that they don’t fear us the way they do now. Now everything has changed, there is treatment, there is prevention. An HIV diagnosis should not be a guilty verdict—it’s just a diagnosis.”
Most countries in the eastern Europe and central Asia region have criminal penalties and various types of punishment, including imprisonment, for concealing a source of HIV infection, for putting someone at risk of HIV or for transmitting HIV. HIV criminalization disproportionately affects marginalized populations, especially women. Women are more likely to find out their HIV status when accessing health care, such as for pregnancy, and are more likely to be criminalized and punished.
“We know for certain that laws that criminalize HIV are counterproductive, undermining rather than supporting efforts to prevent new HIV infections. We hope that by consolidating the efforts of governments and public organizations it will be possible to revise outdated laws in the near future, taking into account the latest data on HIV, which will allow people living with HIV, or those who are most at risk of infection, to be open in their relationships with medical organizations, to disclose their HIV status and use affordable medical services,” said Eleanora Hvazdziova, Director, a.i., of the UNAIDS Regional Support Team for Eastern Europe and Central Asia.
[Feature] It Takes More Than A Village to End HIV Criminalisation
The proverb says, “It takes a village to raise a child”. But what if a mother in the village is living with HIV, and some of the villagers stigmatise her? What if that stigma creates a situation where the mother living with HIV is unjustly criminalised because of her HIV status? Then it takes more than a village to get justice for that woman. It takes a global movement to end HIV criminalisation to sensitise and train lawyers and expert witnesses. It takes national communities of women living with HIV to support that woman following her release, and to educate the community in which she lives about HIV.
Introduction
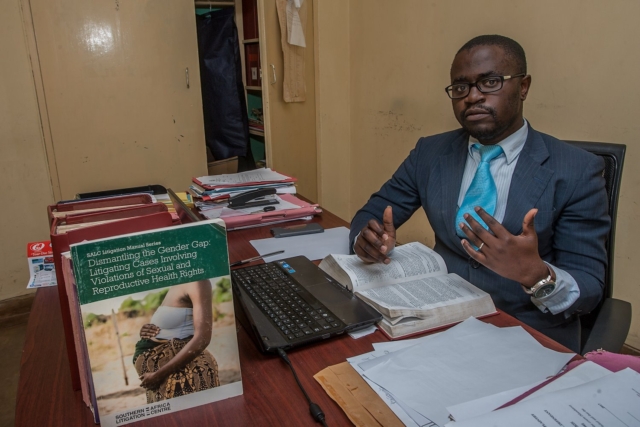
In 2016, a Malawi court convicted a woman living with HIV of “negligently and recklessly doing an act likely to spread the infection of any disease which is dangerous to life” under section 192 of the Malawi Penal Code. She had attended a village meeting with her baby which she breastfed as usual before passing the child to her grandmother. Another woman then asked her to hold her baby. It was alleged that this child began breastfeeding briefly before the woman realised what was happening. The child’s mother then reported the incident to the police. The woman was arrested and without legal advice or representation, pleaded guilty, was convicted, and sentenced to nine months’ imprisonment with hard labour.
In addition, the accused woman was taking antiretroviral therapy. The chances of HIV transmission through even long-term breastfeeding are very low (which is why WHO guidelines recommend it when access to infant formula and clean water are limited) and the chances of transmission during the brief period the baby allegedly fed were infinitesimally small. In fact, the accused woman’s own child, who was routinely breastfed, has not acquired HIV, calling into question any suggestion that she intended to cause harm to the other woman’s child. Perversely, for a system that unjustly condemned her for risking harm to the other woman’s child, her own baby was imprisoned with her, without any arrangements for appropriate feeding and care, negating any notion that the legal system’s purpose was to protect children.
Following media reports of her initial conviction, numerous individuals and organisations – including HJN and our HIV JUSTICE WORLDWIDE partners, ARASA and SALC – became involved in the case, ultimately changing the outcome for the woman and her family, and laying the groundwork for further anti-HIV stigma advocacy and education in the region. Her story demonstrates the vital role that education, training, strong networks, and community play in the pursuit of HIV justice.
Living with HIV-related stigma
When interviewed at her home in 2019, the woman referred to as “EL” talked about her life:[1]
[1] The initials EL are used instead of her full name following a court order of anonymity to protect her privacy. The interview took place in 2019, during the village visit described later in this article.
“As kids, there were the two of us — me and my brother. My parents faced challenges raising us. Finding the basic necessities like soap and food was a tall order, let alone talking about going to school. It was difficult to get learning materials as well as proper clothes to wear at school. I worked hard in class but couldn’t get past Standard 5 at primary school. Eventually I dropped out, and my brother did the same, … My daily life was taken up doing house chores just like any other girl in the village, as well as helping my parents with farming. At 16, I got married.”
EL further described how she was diagnosed HIV-positive in 2015 after a de facto compulsory HIV test at an antenatal visit. She already had two children and was pregnant with her third. She had heard about HIV but did not know much about it. EL said that the healthcare workers provided a lot of assistance, giving her accurate information about HIV, including the importance of adhering to her antiretroviral treatment (ARVs).
EL and two of her children. Photo: Amos Gumulira/UNDP Malawi
EL said that she generally enjoyed life in her village, although at times she was subject to stigma and discrimination:
“When I went to fetch water at the community borehole, people would laugh at me, and whenever I wanted to participate in community work, you would find pockets of community members talking ill about me. Some people used to insult me, calling me names. But I persevered because my relatives, including the Village Headman himself, gave me support and always stood by my side.”
Members of EL’s family also faced discrimination. “Due to lack of information, a lot of people thought HIV was hereditary and because I was diagnosed HIV-positive, this meant that all my family members had HIV, and they were discriminated against,” EL said.
EL wonders if more could have been done to help her fight stigma. In particular, EL gained a lot of knowledge about HIV from the counselling she got when diagnosed, but perhaps she could have been better equipped with information to share with people in her community:
“A lot of people don’t know that if you adhere to ARVs, you reduce the risk of transmitting HIV to others. This information needs to be passed on to many people. There are also other issues to do with ARVs. A lot of people don’t have adequate information on the effects of ARVs and at the end of the day, they start pointing fingers at each other, giving people room to start speculating about issues to do with witchcraft.”
EL’s prosecution had repercussions for her whole village. One woman from the community explained:
“I was there and very close to where EL was sitting. Yes, she was carrying another woman’s child. This other woman had given the child to EL for safe keeping while she went to stand in a queue, but honestly speaking, I didn’t see EL breastfeed the child. I just heard some people who were sitting a distance from where we were sitting, as they started pointing accusing fingers at her.”
She said that things moved so fast that before they could think of anything to stop what she called “the rumour.” It had gotten out of hand and people started saying that EL had intentionally breastfed the child to transmit HIV.
After receiving a summons, EL voluntarily turned herself in at the police station. She was accompanied by the Village Headman (her grandfather) who wanted first-hand information about what crime she was alleged to have committed. That same day, police transferred EL to a larger town, where she was remanded for three days. At the age of 29, this was the first time that EL had ever left her village.
Days later, she appeared in court and the charge sheet was read out. EL recounted that she had not understood what was happening and could not make arguments because she had no legal representation. EL agreed with the summary of events as they were described, so she was found guilty and was imprisoned together with her youngest child.
She described life in prison as “hell”:
“After a week, my brother showed up to give me my ARVs. All this talk about a woman with HIV breastfeeding. I breastfed but I also found it tough to feed my baby while in prison because there was no provision of special food for babies. We were eating nandolo (pigeon peas) almost every day with Msima ya Mgaiwa (maize meal). And there was only one toilet for a cell of more than 50 people.”
After some time, relatives and other members of her community started visiting, giving her money she could use to buy soap and food for her baby. “When we heard from our Village Headman that she had been arrested, we were so devastated”, a woman from EL’s village explained. “We raised funds for some members to go and give her support only to learn that she had been transferred to one town, then another, but some of us did manage on several occasions to visit her and offer our support when she was in prison.”
Then, out of the blue, EL received a message that some people had come looking for her. She went to meet them: a lawyer, Wesley Mwafulirwa, and his paralegal. They explained why they were there and asked if she would like them to appeal on her behalf. She accepted enthusiastically. “I was excited but at the same time I was confused because I could not believe that I could be so lucky to have these people come to help me.”
Fighting the charges
Solicitor Wesley Mwafulirwa had volunteered to attend training to address legal barriers to prison health and human rights presented by the Southern African Litigation Centre (SALC). He travelled from Malawi to South Africa to attend the training which addressed useful regional and international mechanisms, and presented insights about legal practice and strategic litigation to support prison health and human rights, particularly for those facing heightened vulnerability to HIV and TB.
At the training, two lawyers spoke about their pro bono work. Wesley remembers one of them, Allan Maleche (Executive Director of KELIN), saying that each participant should take at least one case when they go back to their country. It was a turning point in Wesley’s career.
He had not been home long when he saw an article in the newspaper about an HIV-positive person convicted for trying to spread HIV. That person was EL.
Wesley, who lives in a small town in northern Malawi, drove for more than ten hours to get to the jail where EL was incarcerated. He explained his determination, saying “I was so fired up! I’d just come from SALC’s training … and I said, ‘I want to take up this case’.”
Wesley interviewed EL and offered to take her case pro bono. Wesley contacted SALC, who offered technical support. Their first step was to get an order for anonymity to protect EL’s identity and gain greater control over media reporting. Next, they faced an ethical question. They wanted to challenge the constitutionality of the law but that would take a long time. Because EL was in prison, they decided to undertake a criminal appeal instead. They applied for EL to be let out of custody on bail pending appeal. This is usually a difficult application to win, but they were successful and EL was released from prison.
In the appeal, the court was asked to consider whether the conviction could be justified, whether the penal provision was constitutional (arguing it was overly broad and vague), and whether the sentence was manifestly unjust. Wesley used his learnings from the SALC training to raise international principles and instruments relating to sentencing, which the court referenced and upheld. Michaela Clayton, then Executive Director of the AIDS and Rights Alliance for southern Africa (ARASA), and now a member of HJN’s Supervisory Board, provided expert testimony. Another expert witness, Dr Ruth Brand, identified through HJN’s global network, gave expert scientific evidence to show the risk of HIV transmission had been “infinitesimally small.”
The case was heard by Honourable Justice Zione Ntaba, who held that the proceedings in the trial court were irregular and “blatantly bias” against EL, compromising her right to a fair trial. Justice Ntaba found the charge sheet had been defective and therefore EL’s plea should not have been recorded as guilty. She noted the law must be sensitive to the accused’s knowledge or belief (or lack of) that HIV would be transmitted. Justice Ntaba decided the conviction could not be justified, acknowledging human rights principles against the overly broad criminalisation of HIV non-disclosure, exposure, or transmission. EL’s sentence was set aside. (The Constitutional challenge was referred to a full-member panel of the Constitutional Court although the case was not pursued.)
Notably, Justice Ntaba was a member of the African Regional Judges Forum to discuss HIV, TB and Human Rights (a process which is owned and planned by the judges and run with support from UNDP and funding from the Global Fund).
Fighting the stigma
Shortly after EL’s arrest, the Coalition of Women and Girls Living with HIV and AIDS in Malawi (COWLHA) and the Malawi branch of the International Community of Women Living with HIV/AIDS (ICW-Malawi) discussed the case at a roundtable meeting. At first, everyone was surprised and even laughed, questioning how she could have breastfed someone else’s child. They had never heard of a criminal case involving infant feeding and did not understand what they were dealing with.
During their discussions, COWLHA and ICW-Malawi agreed that the prosecution of EL was a manifestation of stigma and misinformation about HIV in the community. They learned more about the unjust measures that EL had experienced, like being imprisoned without being given a chance to be heard and not being given the chance to prepare and take her medication and things she needed to care for her child. COWLHA and ICW decided to get involved.
Representatives from COWLHA and ICW meet with members of EL’s village. Photo: COWLHA/ICW
Concerned that EL could face social and community hostility after her release, COWHLA and ICW planned a visit to the village to provide psychosocial support to EL and to work with traditional community leaders to provide community sensitisation on HIV, addressing issues of stigma and discrimination. Their efforts helped change some community members’ ideas about HIV.
The community formed two support groups— one for youth and another for adults (notably both were predominantly female groups). They have conducted numerous activities, including home visits, supporting children to go to school, helping the elderly with house chores, and they have a garden where they grow vegetables and rice. They hoped to access loans to become self-reliant. They also had a list of issues they wanted to learn more about, including preventing mother-to-child transmission, sexual and reproductive health, positive living, stigma and discrimination, and treatment literacy.
Visiting EL at home
In September 2019, a three-member team comprising Edna Tembo (Executive Director of COWLHA), Charity Mkona (ICW Board Chair), and Peter Gwazayani (media consultant), set out for EL’s village.
The team was welcomed by the Group Village Headman, who took them to EL’s house. EL recognised Edna from the work COWLHA and ICW-Malawi had done in the community previously. EL welcomed the team with a big smile.
EL and her husband looked cheerful as they laid a mat on the veranda of their house for the visitors. Her mother later joined the discussion.
EL was interested to learn that HJN wanted to write about her case and the type of interventions that had been helpful, to share the story with advocates for HIV justice around the world.
EL recounted that when she returned to the village, “most members of my community received me with happiness, particularly my relatives. The day I arrived, they were jubilant. They celebrated with songs that we normally sing during special occasions in the village.”
COWLHA ED Edna Tembo and Charity Mkona of ICW chat with EL, her husband and her mother (at far distance). Photo: COWLHA/ICW
EL lives with her husband, five children and her mother in a compound made up of three grass thatched houses. She introduced her children:
“The oldest is 13 and she goes to school, as do the second and third. The fourth, a little girl, is the child I was with in prison. She has not yet started school. And then there is this one, who I am breastfeeding. She is the fifth one. She has been tested for HIV on two occasions and will be going for the last test soon. The other two tests have come back HIV-negative.”
EL’s accuser and her family still lives in the same village which has presented some difficulties. EL said that on several occasions she had tried to greet them when they passed each other, but she had been ignored. “They don’t talk to me but from deep down in my heart, I have no grudges against them,” EL said. “I am just living my normal life,” EL says, although now she says that she would never agree to carry anybody else’s child, for any reason.
Moving beyond criminalisation
With respect to the community-level interventions, lawyer Annabel Raw, who worked at SALC during the time they supported the EL case said:
“As lawyers, we would never have thought to consider such an intervention had ICW-Malawi and COWLHA not shared their insights and been willing to support the client and her community. Their work has been so important to ensuring that meaningful justice was done to combat the actual root cause of the prosecution — stigma and discrimination — and to reconcile EL with her community.”
Engaging with the community also influenced ICW-Malawi and COWLHA’s thinking about HIV criminalisation. COWLHA’s Edna Tembo noted that:
Supporting people who have been prosecuted, particularly women, gives them power, … However, it is very important to stress that psychological support is absolutely vital for those who have been prosecuted. That includes family support, and a supportive community environment enabling acceptance of an individual accused.”
Tembo was also quick to emphasise that there is more work to be done. That work includes awareness raising and ongoing support to the community, especially to identify and train volunteers, empowering them to provide services at community level and to link them to health facilities and district offices for continued support and mentorship.
EL carries her youngest child home. Photo: Amos Gumulira/UNDP Malawi
EL described her dreams for the future:
“My wish now is to see my children progress in school so that they become productive citizens in this community and help it grow. That’s my dream. If they get educated, they will be able to stand on their own and support others. My husband is not employed and it is a challenge to get money for school fees for our children. We would love to get a loan or training to have greater knowledge of economic empowerment because we want to be self-reliant. We would then love to lease some land to grow rice to sell to pay back the loan.
“It’s also my wish to see the lives of all people in the community uplifted. We farm but on a small-scale. If we were to be supported with funds, I’d love to see the community establish big rice farms, working in groups, harvesting for consumption and for sale. In so doing, we would be able to uplift our lives for the better.”
Further Information
Learn more about Wesley’s experiences in EL’s case here and here.
Learn more about the African Regional Judges Forum here.
The full High Court judgement is available here, with a summary included here.
Read more about the successful HIV and AIDS Management Act community advocacy here.
This article is based on information provided by ICW-Malawi and COWLHA following their visits to EL’s village, and an interview with Wesley Mwafulirwa published by UNDP. HJN provided financial and logistical support for the village visits thanks to a grant provided to the HIV Justice Global Consortium from the Robert Carr Fund for civil society networks.
The Importance of Human Kindness and Connection: Sero’s Holiday Card Project
In an era where the term ‘lockdown’ is used to limit our movements, spare a thought for the many prisoners living with HIV (some of whom have been unjustly convicted under HIV criminalisation laws) who are experiencing real lockdowns and severe isolation.
With community support interventions becoming increasingly formalised, and NGOs pushed to operate in terms of strategic plans, deliverables, outputs and outcomes, Sero’s Holiday Card Project stands as a rare example of an organisation recognising the worth of a project focused solely on gestures of basic human kindness.
Last year, the project delivered Holiday cards to around 900 incarcerated people, most of whom are living with HIV. For some, it was the only mail they received all year.
So how did the Holiday Card Project come to be, has it made a difference, and how can you help this year?
Back in the 1980s and ’90s, Cindy Stine lost a lot of friends to HIV. In 1996, just before effective treatments became available, she lost a close friend who was like a son. She made a promise to him that she would continue to be involved in the AIDS response. That’s a promise she’s kept.
Cindy Stine of the Sero Project
In 2011, Cindy was serving on the board of a local LGBT centre when she invited two speakers from the fledgling Sero Project to speak at an event. The speakers were Sean Strub, Sero’s Executive Director, and Robert Suttle. Sean introduced the audience to the concept of HIV criminalisation, a new issue for most, including Cindy. Robert talked about what it means to live as an HIV criminalisation survivor, explaining that as the result of an HIV non-disclosure charge, he served six months in the Louisiana state prison and would be registered as a sex offender for 15 years. Robert showed an image of his driver’s license, with ‘sex offender’ stamped in bold red lettering: ID he has to show often and in many different circumstances.
Cindy approached Sean and Robert to let them know that she wanted to help. A few days later, Sean rang Cindy and invited her to his office where he showed her a stack of letters that Sero had received from people in prison. Sean asked Cindy if she’d volunteer to take on the task of answering the letters. She agreed.
Things could have ended there, with Cindy answering people’s individual letters, but as Cindy read those letters week after week, each letter more heart-breaking than the last, she began to really appreciate the isolation, loneliness and desperate need for connection experienced by many of those inside. She talked it over with her Sero colleagues, and they decided their efforts to build a movement against HIV criminalisation needed to expand to be more inclusive of those who were incarcerated; those directly impacted by HIV criminalisation. They decided to explore how they could support development of a prisoners’ network, starting by compiling a database of contact details of those who’d written.
As Sero grew, Cindy was employed to take on community education and other projects but her work answering prisoners’ letters continued. Cindy says of those letters, “sometimes the people writing didn’t even have access to paper, so they’d write on any scrap of paper they could find – recycled envelopes or bits of paper torn off something else. Many of those sending letters weren’t really literate but they wanted to communicate.”
As the 2015 Holiday season approached, Cindy found the letters got harder to read. “A lot of people wrote about loneliness and about their families disowning them after finding out they had HIV, or were gay, or were transgender. People felt they’d been thrown away and forgotten.” Then she had a simple thought, “Wouldn’t it be nice for them to know that they’re not alone.” Then another, “We should send Holiday cards”. She took the idea to Sean, who agreed.
By then, Cindy’s database was so large that she realised Sero would need to prioritise who got cards, focusing on those who were incarcerated as a result of HIV, or they had HIV or another debilitating illness. Cindy also wanted to ensure each person got at least three or four cards but … how to go about it? Cindy put out a call to the 900 or so people on the Sero list-serve asking if anyone was interested in writing some Holiday cards. The response was overwhelming. Many offered to help, with some asking to do 20 cards, some asking to do 200.
The Holiday Card Project has continued each year since then. People express an interest, Cindy sends them a list of first names; they write message on the cards, put them in blank envelopes and return them to Sero; Cindy sorts them, addresses them, and mails them off.
Those who write cards come from all different parts of the community, including some working in other HIV advocacy organisations, some parents of prisoners, and some people living with HIV. People are asked not to ask personal questions but to write messages of support: things like ‘hope you’re doing well’, ‘we’re thinking of you’, and ‘you’re not forgotten’. Some write about themselves, their experience living with HIV, their thoughts and prayers. Some write, ‘we’re thinking of you when we fight HIV criminalisation’.
Sero’s staff and volunteers
One group gets together and spends a day each year writing Holiday cards. People come from all over, saying it feels really good coming into a non-judgemental space and writing messages from the heart. Sometimes Sero will set up a table at a conference and invite people to write cards. Others write cards at home. People feel involved. Each step in the process has meaning: the choice of card, the choice of words, with many people sending their cards with stamps to send them on, to further support the project.
Last Holiday season, about 900 people received cards in facilities across the US, including people on death row. The responses from those who received cards is humbling. Some said, it was the only card they’d received all year, but those cards meant that they knew they were not forgotten. They couldn’t describe the feeling of hearing someone from the mailroom say, ‘You’ve got mail’. They knew that somebody out there had thought enough of them to send a card. Recently Cindy received a letter from a man who’s recently been released. He said that for the last three years he’d so looked forward to those cards as it was the only mail he got. It meant a lot that people had taken the time to write.
The project is not without its challenges. Cindy spends considerable time keeping track of people, as prisoners are often moved. There are also major issues regarding mail screening. Although Cindy has worked to build a rapport with those managing mail distribution at many of the prisons, that hasn’t guaranteed mail is always received. Mail screening rules differ from state to state, institution to institution, and the rules keep changing. Some prisons have now banned cards altogether, some won’t allow glue or glitter or coloured paper, etc. If mail is considered contraband it may be thrown out or returned to Sero. That process has at times driven Cindy to photocopy returned cards, sending the copies in the hope the person will still receive the good wishes.
The Holiday Card Project may have modest goals – to show compassion and care to those who feel abandoned, but it has delivered far more. It has made a difference to the lives of many, letting them know that there are people outside of prison ready to provide support. It has raised awareness about HIV criminalisation and provided a mechanism for people to show they care. It has also helped build trust between prisoners and Sero, a facor that has proven critical to the development of a stronger prisoners’ network and greater engagement with Sero. A stronger prisoners’ network has meant more support for those inside, and it has also resulted in other great projects, like Turn It Up, the health magazine that includes information about HIV for those in prison, largely written by people who are, or have been, incarcerated.
Some of Sero’s Holiday cards
While Sero is best known for its HIV criminalisation reform programmes, its efforts to support network building and empowerment have proven equally important. Sero operates from the belief that those most directly impacted should be at the centre of this work, which is why facilitating the creation and strengthening of networks of People Living with HIV and allies, particularly those representing key populations, remains critical and a priority.
Every year the Holiday Card Project has grown, with prisoners writing to Cindy to let her know if they’ve been moved to another facility. Others write saying, “a friend of mine got cards. Can I be put on the list?” Parents get in touch too, asking for their children to be added to the list, and also writing letters of thanks for cards received.
Still, Cindy thinks there is room for the project to grow; sending cards for holidays celebrated by other religions at other times of the year, and also considering whether cards could be sent for some non-religious events, such as Halloween or Thanksgiving. That way the project can become more inclusive and people won’t have to wait an entire year for mail. Of course, that will mean attracting more people to write cards so that more people can receive them.
If you’re interested in supporting the work of the Holiday Card Project, please contact Cindy at cindy.stine@seroproject.com, Subject – Holiday Card Project.
Watch all the videos of Beyond Blame @HIV2020 – our “perfectly executed…deftly curated, deeply informative” webshow
Earlier this month, advocates from all over the world came together for two hours to discuss the successes and challenges of the global movement to end HIV criminalisation.
All of the recordings of Beyond Blame: Challenging HIV Criminalisation for HIV JUSTICE WORLDWIDE are now available on the HIV Justice Network’s YouTube Channel.
Kene Esom, Policy Specialist: Human Rights, Law and Gender, United Nations Development Programme (UNDP)
The full-length director’s cut version – with enhanced audio and video – is now available in English as well as with the audio track of the recorded simultaneous translation in French, Spanish, Russian, and Portuguese.
“We have been being battling this fight for many years. Since the start of the HIV epidemic we as gay men, as gay women, as queers, as transgender people, as sex workers, as people using drugs, have been persecuted by the criminal law. And I’m here to say, “Enough! Enough!
We have achieved a great deal with our movement, with the HIV Justice Network. We have achieved a great deal in conscientizing law makers, law givers and the public. It is now time for us to join in unison to demand the end of these stigmatising, retrograde, unproductive, hurtful, harmful laws.
It is a long struggle we’ve engaged in. And it’s one that has hurt many of us. Some of us here today, some of us listening in, some of us who have spoken, have felt the most brutal brush of the law. They have been imprisoned, unjustly prosecuted, unjustly convicted, and unjustly sent away.
HIV is not a crime. But there is more to it. Criminalising HIV, criminalising the transmission or exposure of HIV, as many countries on my own beautiful continent Africa do, is not just stupid and retrograde. It impedes the most important message of the HIV epidemic now, which is that this epidemic is manageable. I’ve been on antiretroviral treatment now for very nearly 23 years. My viral load has been undetectable for more than 20.
We can beat this, but we have to approach this issue as public health issue. We have to approach it rationally and sensibly, and without stigma, and without targeting people, and without seeking to hurt and marginalise people.We’ve made calamitous mistakes with the misapplication of the criminal law over the last hundred years, in the so-called ‘war on drugs’. We continue to make a calamitous mistake in Africa and elsewhere by misusing the criminal law against queer people like myself. We make a huge mistake by misusing the criminal law against people with HIV.
Let us rise today and say, “Enough!”
You can select your preferred language from the 'Select Language' menu at the top of the page.
Continue
We use cookies to ensure that we give you the best experience on our website. By continuing to use our site, you are agreeing to our use of cookies. You can change your cookie settings at any time if you want. Find out more in our Privacy & Cookie Policy.