HIV criminalization is not a new concern. For decades, people living with HIV in Canada have faced the reality that they can still face public outing by authorities, prosecution by the “justice” system, and imprisonment for allegedly not disclosing their HIV status to a sexual partner. This continues to be the case today, even in situations where there was no realistic possibility of transmission, no intent to transmit, and no transmission actually happened.
And for decades, people living with HIV, activists and community advocates, legal minds, and public health and medical experts have shown again and again that Canada’s terribly punitive approach is discriminatory, scientifically outdated, and harmful to public health. It reinforces and codifies systemic injustices and inequalities based on race, migration status, sexual orientation, and gender. It contradicts current science on HIV transmission, and it entrenches HIV stigma, further cementing barriers that people living with HIV face to accessing care and treatment, not to mention housing, employment, and personal safety. How can we expect people to feel safe getting tested and learning their HIV status when it could later be vindictively used against them?
That’s why it really mattered when, on December 1st, 2017, the Government of Canada acknowledged these very concerns and highlighted the problematic state of HIV criminalization on World AIDS Day in their report Criminal Justice System’s Response to Non-Disclosure of HIV. The problem is that since 2017, the government’s actions have not caught up to words and there has been little progress from Canada to right these wrongs. People living with HIV in this country continue to be forced to live in fear.
Over the last eight years, activists, led by people living with HIV themselves, have continued to move the needle on HIV criminalization. Thanks to their efforts, the federal government announced national consultations on HIV criminalization at the 2022 International AIDS Conference, which was held in Montreal. “Our government recognizes that the criminalization of people living with HIV can lead to stigmatization and significant hardships,” stated then-Minister of Justice David Lametti. “This is why we are consulting Canadians on the best approach to reform the criminal law regarding HIV non-disclosure. It will help us find solutions, and will lead to better outcomes for affected populations.”
Those consultations concluded in early 2023 and since that time, no law reform has been introduced. Productive meetings with advocates aimed at making meaningful change continued for a time, until the Government of Canada quietly informed us last year that it had put any plans for real justice on the backburner.
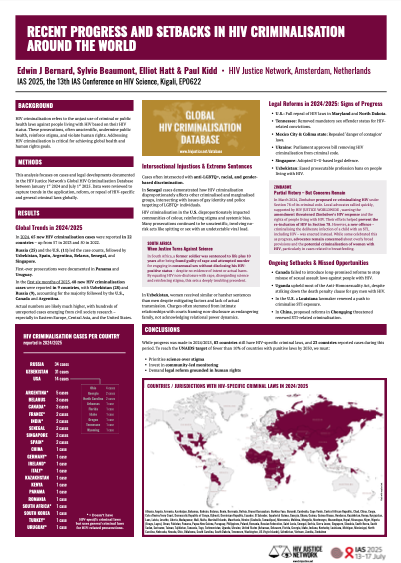
While other jurisdictions, including various American states, such as Nevada, Virginia, Maryland, and Illinois, narrow or eliminate misguided prosecutions, the threat of criminalization continues to hang over the heads of people living with HIV here in Canada. In parallel, at a time when fewer people are being diagnosed with HIV around the world, HIV cases rose a staggering 35.2% in Canada between 2022 and 2023. While preliminary data from 2024 indicate a slight decrease in new cases in Canada, only time will tell whether this represents a reversal from recent worrying trends. What remains clear is that Canada must do more – both in its legal and policy responses – to get back on track toward the goal of eliminating HIV as a public health threat by 2030.
And so, every World AIDS Day, advocates find themselves writing yet another op-ed urging Canada to act. The headlines over the past few years alone tell the story: “Unjust HIV Criminalization is a National Disgrace”; “The Government of Canada Must Act to End the Harms of HIV Criminalization”; “We Need to Stop Criminalizing People with HIV”; “Let’s Stop Criminalizing HIV Status.” How long until these headlines are finally replaced with news that Canada has followed through on its promises to end the harms of HIV criminalization?
With a new government in place, we are feeling more hopeful than we were last World AIDS Day. But this government still needs to take firm and decisive action to bring Canada’s laws in line with science and human rights, and remove the stigma and discrimination against people living with HIV that is currently entrenched in our justice system. In so doing, we could envision a very different headline for next year’s World AIDS Day op-ed, and a very different reality for people living with HIV in Canada.
Muluba Habanyama is the Chair of the Canadian Coalition to Reform HIV Criminalization
Colin Hastings is an Assistant Professor at the University of Waterloo
André Capretti is a Policy Analyst at the HIV Legal Network