This week, our close partners in the HIV JUSTICE WORLDWIDE coalition, the Canadian-based HIV Legal Network, published a thought-provoking new report, A gender-centred dialogue on alternative justice responses to HIV non-disclosure criminalization in English and French.
Whilst the report focuses on the specifics of the Canadian situation, it provides for provocative and stimulating reading that should inspire all of us working to end HIV criminalisation and other punitive approaches to HIV prevention.
Funded by Women and Gender Equality (WAGE) Canada, the brief synthesises and builds upon the roundtable that was co-hosted by the HIV Legal Network with the Women & HIV/AIDS Initiative (WHAI) and Communities, Alliances & Networks (CAAN) in June 2022.
The objective of the roundtable was to gather cross-sector perspectives about whether an alternative justice approach is warranted or appropriate in situations of HIV non-disclosure.
Given the unique legal situation in Canada, where HIV non-disclosure is prosecuted as sexual assault, and given the interaction between HIV criminalisation, disclosure, and gender – including the risks of gender-based violence and gendered power dynamics – the discussions were grounded in gender-centred considerations.
Since most alternative justice responses focus on repairing the harm caused by an individual and include holding people accountable for their actions, the roundtable and the report raised questions around applying the notions of “harms” or “wrongdoing” to HIV non-disclosure.
Is HIV non-disclosure a harm in and of itself? Or does it depend on the circumstances and characteristics of the involved parties?
Given its harmful impacts, there was a consensus among participants that the criminal law is not the appropriate instrument to respond to HIV non-disclosure.
To respond to the needs of people who experience non-disclosure and account for the realities of women and gender-diverse people including those living with HIV, roundtable participants discussed potential alternative responses, including restorative and transformative justice models.
The roundtable and the report also focused on community-based alternatives to the criminal legal system, notably how to foster collaboration between the HIV sector, the sexual assault and gender-based violence sector, and alternative justice organisations.
Three main themes on alternative community-based interventions emerged from the roundtable:
1. Creating enabling environments for positive and healthy sexuality and sexual relationships.
2. Delivering dynamic, non-shame-based, responses to situations of non-disclosure that depend on the needs of the parties and communities involved.
3. Recognising that an alternative justice approach to HIV non-disclosure must be one that transforms the conditions that lead to increased HIV vulnerability and experiences of violence and criminalisation, all of which must be grounded in an anti-racist and anti-colonial approach.
The report concludes that the current state of HIV criminalisation is untenable and fails to promote “justice” for anyone involved. It ends with a number of recommendations from the HIV Legal Network aimed at the federal government, public health departments, and HIV-impacted communities that primarily focus on creating a supportive, enabling environment for HIV prevention, treatment, care and support.
You can find A gender-centred dialogue on alternative justice responses to HIV non-disclosure criminalization in the English and French versions of the Resource Library of the HIV Justice Academy, as well as on the HIV Legal Network‘s website.
[Feature] It Takes More Than A Village to End HIV Criminalisation
The proverb says, “It takes a village to raise a child”. But what if a mother in the village is living with HIV, and some of the villagers stigmatise her? What if that stigma creates a situation where the mother living with HIV is unjustly criminalised because of her HIV status? Then it takes more than a village to get justice for that woman. It takes a global movement to end HIV criminalisation to sensitise and train lawyers and expert witnesses. It takes national communities of women living with HIV to support that woman following her release, and to educate the community in which she lives about HIV.
Introduction
In 2016, a Malawi court convicted a woman living with HIV of “negligently and recklessly doing an act likely to spread the infection of any disease which is dangerous to life” under section 192 of the Malawi Penal Code. She had attended a village meeting with her baby which she breastfed as usual before passing the child to her grandmother. Another woman then asked her to hold her baby. It was alleged that this child began breastfeeding briefly before the woman realised what was happening. The child’s mother then reported the incident to the police. The woman was arrested and without legal advice or representation, pleaded guilty, was convicted, and sentenced to nine months’ imprisonment with hard labour.
In addition, the accused woman was taking antiretroviral therapy. The chances of HIV transmission through even long-term breastfeeding are very low (which is why WHO guidelines recommend it when access to infant formula and clean water are limited) and the chances of transmission during the brief period the baby allegedly fed were infinitesimally small. In fact, the accused woman’s own child, who was routinely breastfed, has not acquired HIV, calling into question any suggestion that she intended to cause harm to the other woman’s child. Perversely, for a system that unjustly condemned her for risking harm to the other woman’s child, her own baby was imprisoned with her, without any arrangements for appropriate feeding and care, negating any notion that the legal system’s purpose was to protect children.
Following media reports of her initial conviction, numerous individuals and organisations – including HJN and our HIV JUSTICE WORLDWIDE partners, ARASA and SALC – became involved in the case, ultimately changing the outcome for the woman and her family, and laying the groundwork for further anti-HIV stigma advocacy and education in the region. Her story demonstrates the vital role that education, training, strong networks, and community play in the pursuit of HIV justice.
Living with HIV-related stigma
When interviewed at her home in 2019, the woman referred to as “EL” talked about her life:[1]
[1] The initials EL are used instead of her full name following a court order of anonymity to protect her privacy. The interview took place in 2019, during the village visit described later in this article.
“As kids, there were the two of us — me and my brother. My parents faced challenges raising us. Finding the basic necessities like soap and food was a tall order, let alone talking about going to school. It was difficult to get learning materials as well as proper clothes to wear at school. I worked hard in class but couldn’t get past Standard 5 at primary school. Eventually I dropped out, and my brother did the same, … My daily life was taken up doing house chores just like any other girl in the village, as well as helping my parents with farming. At 16, I got married.”
EL further described how she was diagnosed HIV-positive in 2015 after a de facto compulsory HIV test at an antenatal visit. She already had two children and was pregnant with her third. She had heard about HIV but did not know much about it. EL said that the healthcare workers provided a lot of assistance, giving her accurate information about HIV, including the importance of adhering to her antiretroviral treatment (ARVs).
EL and two of her children. Photo: Amos Gumulira/UNDP Malawi
EL said that she generally enjoyed life in her village, although at times she was subject to stigma and discrimination:
“When I went to fetch water at the community borehole, people would laugh at me, and whenever I wanted to participate in community work, you would find pockets of community members talking ill about me. Some people used to insult me, calling me names. But I persevered because my relatives, including the Village Headman himself, gave me support and always stood by my side.”
Members of EL’s family also faced discrimination. “Due to lack of information, a lot of people thought HIV was hereditary and because I was diagnosed HIV-positive, this meant that all my family members had HIV, and they were discriminated against,” EL said.
EL wonders if more could have been done to help her fight stigma. In particular, EL gained a lot of knowledge about HIV from the counselling she got when diagnosed, but perhaps she could have been better equipped with information to share with people in her community:
“A lot of people don’t know that if you adhere to ARVs, you reduce the risk of transmitting HIV to others. This information needs to be passed on to many people. There are also other issues to do with ARVs. A lot of people don’t have adequate information on the effects of ARVs and at the end of the day, they start pointing fingers at each other, giving people room to start speculating about issues to do with witchcraft.”
EL’s prosecution had repercussions for her whole village. One woman from the community explained:
“I was there and very close to where EL was sitting. Yes, she was carrying another woman’s child. This other woman had given the child to EL for safe keeping while she went to stand in a queue, but honestly speaking, I didn’t see EL breastfeed the child. I just heard some people who were sitting a distance from where we were sitting, as they started pointing accusing fingers at her.”
She said that things moved so fast that before they could think of anything to stop what she called “the rumour.” It had gotten out of hand and people started saying that EL had intentionally breastfed the child to transmit HIV.
After receiving a summons, EL voluntarily turned herself in at the police station. She was accompanied by the Village Headman (her grandfather) who wanted first-hand information about what crime she was alleged to have committed. That same day, police transferred EL to a larger town, where she was remanded for three days. At the age of 29, this was the first time that EL had ever left her village.
Days later, she appeared in court and the charge sheet was read out. EL recounted that she had not understood what was happening and could not make arguments because she had no legal representation. EL agreed with the summary of events as they were described, so she was found guilty and was imprisoned together with her youngest child.
She described life in prison as “hell”:
“After a week, my brother showed up to give me my ARVs. All this talk about a woman with HIV breastfeeding. I breastfed but I also found it tough to feed my baby while in prison because there was no provision of special food for babies. We were eating nandolo (pigeon peas) almost every day with Msima ya Mgaiwa (maize meal). And there was only one toilet for a cell of more than 50 people.”
After some time, relatives and other members of her community started visiting, giving her money she could use to buy soap and food for her baby. “When we heard from our Village Headman that she had been arrested, we were so devastated”, a woman from EL’s village explained. “We raised funds for some members to go and give her support only to learn that she had been transferred to one town, then another, but some of us did manage on several occasions to visit her and offer our support when she was in prison.”
Then, out of the blue, EL received a message that some people had come looking for her. She went to meet them: a lawyer, Wesley Mwafulirwa, and his paralegal. They explained why they were there and asked if she would like them to appeal on her behalf. She accepted enthusiastically. “I was excited but at the same time I was confused because I could not believe that I could be so lucky to have these people come to help me.”
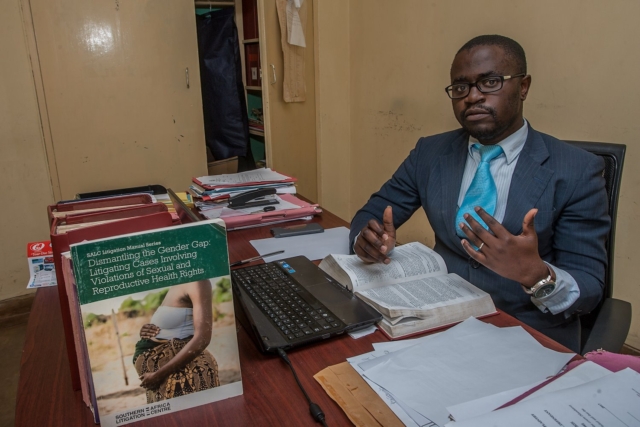
Fighting the charges
Solicitor Wesley Mwafulirwa had volunteered to attend training to address legal barriers to prison health and human rights presented by the Southern African Litigation Centre (SALC). He travelled from Malawi to South Africa to attend the training which addressed useful regional and international mechanisms, and presented insights about legal practice and strategic litigation to support prison health and human rights, particularly for those facing heightened vulnerability to HIV and TB.
At the training, two lawyers spoke about their pro bono work. Wesley remembers one of them, Allan Maleche (Executive Director of KELIN), saying that each participant should take at least one case when they go back to their country. It was a turning point in Wesley’s career.
He had not been home long when he saw an article in the newspaper about an HIV-positive person convicted for trying to spread HIV. That person was EL.
Wesley, who lives in a small town in northern Malawi, drove for more than ten hours to get to the jail where EL was incarcerated. He explained his determination, saying “I was so fired up! I’d just come from SALC’s training … and I said, ‘I want to take up this case’.”
Wesley interviewed EL and offered to take her case pro bono. Wesley contacted SALC, who offered technical support. Their first step was to get an order for anonymity to protect EL’s identity and gain greater control over media reporting. Next, they faced an ethical question. They wanted to challenge the constitutionality of the law but that would take a long time. Because EL was in prison, they decided to undertake a criminal appeal instead. They applied for EL to be let out of custody on bail pending appeal. This is usually a difficult application to win, but they were successful and EL was released from prison.
In the appeal, the court was asked to consider whether the conviction could be justified, whether the penal provision was constitutional (arguing it was overly broad and vague), and whether the sentence was manifestly unjust. Wesley used his learnings from the SALC training to raise international principles and instruments relating to sentencing, which the court referenced and upheld. Michaela Clayton, then Executive Director of the AIDS and Rights Alliance for southern Africa (ARASA), and now a member of HJN’s Supervisory Board, provided expert testimony. Another expert witness, Dr Ruth Brand, identified through HJN’s global network, gave expert scientific evidence to show the risk of HIV transmission had been “infinitesimally small.”
The case was heard by Honourable Justice Zione Ntaba, who held that the proceedings in the trial court were irregular and “blatantly bias” against EL, compromising her right to a fair trial. Justice Ntaba found the charge sheet had been defective and therefore EL’s plea should not have been recorded as guilty. She noted the law must be sensitive to the accused’s knowledge or belief (or lack of) that HIV would be transmitted. Justice Ntaba decided the conviction could not be justified, acknowledging human rights principles against the overly broad criminalisation of HIV non-disclosure, exposure, or transmission. EL’s sentence was set aside. (The Constitutional challenge was referred to a full-member panel of the Constitutional Court although the case was not pursued.)
Notably, Justice Ntaba was a member of the African Regional Judges Forum to discuss HIV, TB and Human Rights (a process which is owned and planned by the judges and run with support from UNDP and funding from the Global Fund).
Fighting the stigma
Shortly after EL’s arrest, the Coalition of Women and Girls Living with HIV and AIDS in Malawi (COWLHA) and the Malawi branch of the International Community of Women Living with HIV/AIDS (ICW-Malawi) discussed the case at a roundtable meeting. At first, everyone was surprised and even laughed, questioning how she could have breastfed someone else’s child. They had never heard of a criminal case involving infant feeding and did not understand what they were dealing with.
During their discussions, COWLHA and ICW-Malawi agreed that the prosecution of EL was a manifestation of stigma and misinformation about HIV in the community. They learned more about the unjust measures that EL had experienced, like being imprisoned without being given a chance to be heard and not being given the chance to prepare and take her medication and things she needed to care for her child. COWLHA and ICW decided to get involved.
Representatives from COWLHA and ICW meet with members of EL’s village. Photo: COWLHA/ICW
Concerned that EL could face social and community hostility after her release, COWHLA and ICW planned a visit to the village to provide psychosocial support to EL and to work with traditional community leaders to provide community sensitisation on HIV, addressing issues of stigma and discrimination. Their efforts helped change some community members’ ideas about HIV.
The community formed two support groups— one for youth and another for adults (notably both were predominantly female groups). They have conducted numerous activities, including home visits, supporting children to go to school, helping the elderly with house chores, and they have a garden where they grow vegetables and rice. They hoped to access loans to become self-reliant. They also had a list of issues they wanted to learn more about, including preventing mother-to-child transmission, sexual and reproductive health, positive living, stigma and discrimination, and treatment literacy.
Visiting EL at home
In September 2019, a three-member team comprising Edna Tembo (Executive Director of COWLHA), Charity Mkona (ICW Board Chair), and Peter Gwazayani (media consultant), set out for EL’s village.
The team was welcomed by the Group Village Headman, who took them to EL’s house. EL recognised Edna from the work COWLHA and ICW-Malawi had done in the community previously. EL welcomed the team with a big smile.
EL and her husband looked cheerful as they laid a mat on the veranda of their house for the visitors. Her mother later joined the discussion.
EL was interested to learn that HJN wanted to write about her case and the type of interventions that had been helpful, to share the story with advocates for HIV justice around the world.
EL recounted that when she returned to the village, “most members of my community received me with happiness, particularly my relatives. The day I arrived, they were jubilant. They celebrated with songs that we normally sing during special occasions in the village.”
COWLHA ED Edna Tembo and Charity Mkona of ICW chat with EL, her husband and her mother (at far distance). Photo: COWLHA/ICW
EL lives with her husband, five children and her mother in a compound made up of three grass thatched houses. She introduced her children:
“The oldest is 13 and she goes to school, as do the second and third. The fourth, a little girl, is the child I was with in prison. She has not yet started school. And then there is this one, who I am breastfeeding. She is the fifth one. She has been tested for HIV on two occasions and will be going for the last test soon. The other two tests have come back HIV-negative.”
EL’s accuser and her family still lives in the same village which has presented some difficulties. EL said that on several occasions she had tried to greet them when they passed each other, but she had been ignored. “They don’t talk to me but from deep down in my heart, I have no grudges against them,” EL said. “I am just living my normal life,” EL says, although now she says that she would never agree to carry anybody else’s child, for any reason.
Moving beyond criminalisation
With respect to the community-level interventions, lawyer Annabel Raw, who worked at SALC during the time they supported the EL case said:
“As lawyers, we would never have thought to consider such an intervention had ICW-Malawi and COWLHA not shared their insights and been willing to support the client and her community. Their work has been so important to ensuring that meaningful justice was done to combat the actual root cause of the prosecution — stigma and discrimination — and to reconcile EL with her community.”
Engaging with the community also influenced ICW-Malawi and COWLHA’s thinking about HIV criminalisation. COWLHA’s Edna Tembo noted that:
Supporting people who have been prosecuted, particularly women, gives them power, … However, it is very important to stress that psychological support is absolutely vital for those who have been prosecuted. That includes family support, and a supportive community environment enabling acceptance of an individual accused.”
Tembo was also quick to emphasise that there is more work to be done. That work includes awareness raising and ongoing support to the community, especially to identify and train volunteers, empowering them to provide services at community level and to link them to health facilities and district offices for continued support and mentorship.
EL carries her youngest child home. Photo: Amos Gumulira/UNDP Malawi
EL described her dreams for the future:
“My wish now is to see my children progress in school so that they become productive citizens in this community and help it grow. That’s my dream. If they get educated, they will be able to stand on their own and support others. My husband is not employed and it is a challenge to get money for school fees for our children. We would love to get a loan or training to have greater knowledge of economic empowerment because we want to be self-reliant. We would then love to lease some land to grow rice to sell to pay back the loan.
“It’s also my wish to see the lives of all people in the community uplifted. We farm but on a small-scale. If we were to be supported with funds, I’d love to see the community establish big rice farms, working in groups, harvesting for consumption and for sale. In so doing, we would be able to uplift our lives for the better.”
Further Information
Learn more about Wesley’s experiences in EL’s case here and here.
Learn more about the African Regional Judges Forum here.
The full High Court judgement is available here, with a summary included here.
Read more about the successful HIV and AIDS Management Act community advocacy here.
This article is based on information provided by ICW-Malawi and COWLHA following their visits to EL’s village, and an interview with Wesley Mwafulirwa published by UNDP. HJN provided financial and logistical support for the village visits thanks to a grant provided to the HIV Justice Global Consortium from the Robert Carr Fund for civil society networks.
It’s Valentine’s Month! February is historically the month of love, and a time to show and share the love.
The HIV Justice Network is pleased to support campaigns in the month of love – February – focusing on HIV-positive living, loving, and justice.
Given the difficulty that some people living with HIV can face when it comes to finding love, including negotiating disclosure, sex for pleasure, and/or creating a family in the context of HIV criminalisation, it is important to acknowledge that everyone is deserving of love and affirmation.
To this end, the HIV Justice Network wishes to acknowledge the following Valentine’s campaigns for and about people living with HIV.
The #LovePositiveWomen campaign is a global initiative running every Feb 1st-14th for each of us to express, share and support women living with HIV or as a friend of the community. It was developed and led by the International Community of Women Living with HIV (ICW), one of seven founding partners of HIV JUSTICE WORLDWIDE.
The campaign uses social media to link local grassroots gestures of love to each other. Using Valentines Day as a backdrop, #LovePositiveWomen “creates a platform for individuals and communities to engage in public and private acts of love and caring for women living with HIV.”
Going beyond romantic love to deep community love and social justice, the campaign is also a call to action. The HIV Justice Network has been supporting this campaign since 2017.
“#LovePositiveWomen is a response to the lack of attention and support and to make commitments. It requires participants to spend time reflecting on how they as either a woman living with HIV or an ally will commit to loving women living with HIV. Through action, change can be made to fueling economies of love and compassion. Working from a place of strength, it focuses on the idea of interconnectedness, relationship building, loving oneself, and loving one’s community. By starting from a place of love, within oneself, there are endless ways that the negative impacts that HIV has on women living with HIV can be lessened.”
#LoveandAccountability Campaign – What are you loving?
Initiated by Accountability International, their annual Valentine’s campaign has focused on a variety of thematic areas including consent, Resolution 275, and challenging criminalisation, among others.
For this year, their focus will feature some key messages around love, advocacy, human rights, justice, and accountability.
“Accountability International is well known for our fun and innovative Valentine’s Day campaigns and our collaborative, diverse, and inclusive way of working, so this year we have decided to put our Valentine’s campaign on steroids.”
Watch out for HJN’s Executive Director to be a part of the campaign, which uses the hashtags #LoveandAccountability and #LoveandHumanRights.
With love,
The HJN Team
US: American Pyschological Association's entire March newsletter explores why HIV criminalisation "can no longer be ignored."
In 2016, the APA joined the ranks of medical and professional organizations opposing HIV criminalization laws (Positive Justice Project Consensus Statement on the Criminalization of HIV in the U.S., n.d.). Since 1986, these laws have criminalized nondisclosure of HIV and engagement in “risk” behaviors (sexual activity, needle sharing, and in some instances spitting and biting) for those who are aware of their HIV status (Lehman, Carr, Nichol, Ruisanchez, Knight, Langford, et al., 2014). Between 1986-2011, 67 HIV-specific criminal laws were enacted in 32 states and two U.S. territories (Lehman, 2014), many or most of which do not consider the level of risk and/or intentionality of the act.
Since the beginning of the AIDS epidemic, hundreds of people living with HIV have been arrested for behaviors posing little, if any, risk of HIV transmission (CDC, 2015). It is estimated that 20-25 percent of prosecuted cases related to HIV exposure/transmission have involved spitting, biting or external exposure to bodily fluids (e.g., throwing bodily fluids) which pose negligible transmission risk (CDC, 2015; Patel, Borkowf, Brooks, Lasry, Lanksy & Mermin, 2014; Pretty, Anderson & Sweet, 2009).
Many HIV-specific criminalization laws were passed before research showed that:
Adherence to antiretroviral therapy results in undetectable viral loads which dramatically reduce HIV transmission (Dieffenbach & Fauci, 2009 [PDF, 119KB]).
People diagnosed with HIV in states with HIV-specific criminal laws must disclose their HIV serostatus to sex partners and injection needle sharing partners and refrain from various sexual behaviors, regardless of actions taken to minimize HIV risk transmission (e.g., consistent condom use, using clean needles, consistent adherence to combination antiretroviral therapy [ART]). In the rare instances in which intentional transmission of HIV is determined, states may use general criminal laws or communicable disease laws to prosecute persons accused of intentionally trying to transmit HIV instead of HIV-specific criminal laws.
Not only do most HIV criminalization laws ignore the level of risk or intentionality of the action, they also do not reflect the current, and considerable, evidence base on HIV transmission (CDC, 2015), and in many instances, they counteract public health efforts to decrease HIV transmission by increasing stigma and discrimination (Valdiserri, 2002). As a result, in 2014, the Civil Rights Division of the Department of Justice issued a “Best Practices Guide to Reform HIV-Specific Criminal Laws to Align with Scientifically-Supported Factors (PDF, 117KB).”
This newsletter will present a human face to HIV criminalization laws and discuss the public health implications and the role that psychological research and practice can play in helping to address the individual and social impact of these laws. By emphasizing this issue, APA strongly encourage states with HIV criminalization laws to repeal such laws and provide psychologists practicing in relevant states with guidance on the impact that HIV-specific laws may have on their clients and the general public’s health.
COESIDA Trained Municipal Police in HIV, AIDS and STIs
To contribute to the full training of Public Safety officers, from 4 to 8 July, staff of the State Council for the Prevention and Control of AIDS (COESIDA) trained around 150 members of the Municipal Police Force in Oaxaca de Juarez, in HIV, AIDS and other sexually transmitted infections. Ofelia Martinez Lavariega, head of the Training Department of COESIDA said that, for the third consecutive year, the workshops were conducted through the Police Academy, in coordination with the Commission for Public Safety, and Traffic and Municipal Civil Protection.
“The goal is to continue the work of awareness, prevention and detection of HIV we have carried on since 2013,” she said, while noting that only last year 120 officers were trained. This year the number of participants grew to 150, reflecting the interest in being trained in issues related to HIV and AIDS, such as masculinity and sensitive language, issues which closed the workshops this year . “This last issue is very important if we consider the characteristics of their work, and the fact that police officers have to deal with key groups – sex workers, trans* people – and that sometimes they do not know how to treat them, and without meaning to, come to violate their human rights, “said Martin Trápaga Sibaja, COESIDA trainer and psychologist.
In 2015, the Commissioner of Public Safety, Traffic and Municipal Civil Protection, José Luis Echeverria Morales, stressed the importance of carrying on with such activities which undoubtedly contribute to the integral training of security forces in the capital’s City Hall. “Today we witness greater interest from public safety officers in the workshops. Initially, the majority had no knowledge about the basic information about HIV, AIDS, about modes of transmission and even about the correct way to put a condom; but now, each time there are more who join the program and also to convey the messages to their peers, take them home and that’s very important, “he said.
In addition to the participation of psychologist Martin Trápaga Sibaja, the police officers were trained by Doctor Angeles Pérez Silva and Psychologist Angelica Castro Pineda, who invited them to exercise their sexuality responsibly and with a shared responsibility.
Capacita COESIDA a policías municipales en materia de VIH, Sida e ITS
A fin de contribuir a la formación integral de las y los elementos de Seguridad Pública, del 4 al 8 de julio, personal del Consejo Estatal para la Prevención y Control del sida (COESIDA) capacitó a alrededor de 150 elementos de la Policía Vial y Municipal de Oaxaca de Juárez, en materia de VIH, sida y otras infecciones de transmisión sexual. Ofelia Martínez Lavariega, jefa del Departamento de Capacitación del COESIDA, indicó que por tercer año consecutivo los talleres se realizan de manera coordinada con la Comisión de Seguridad Pública, Vialidad y Protección Civil Municipal, a través de la Academia de Policía.
“El objetivo es continuar con el trabajo de sensibilización, prevención y detección del VIH que hemos hecho desde 2013”, señaló, al tiempo de destacar que tan solo el año pasado fueron capacitados 120 elementos. Para este año –dijo- el número de participantes creció a 150, lo que refleja el interés por estar informados sobre temas relacionados con el VIH y sida, tales como la masculinidad y lenguaje sensible, con los que se clausuraron los talleres de este año 2016.
“Este último tema es muy importante si consideramos que por las características de su trabajo, las y los policías tienen que lidiar con grupos clave -trabajadoras y trabajadores sexuales o personas trans- a quienes en ocasiones no saben cómo tratar, y sin pretenderlo, llegan a violentar sus derechos humanos”, sostuvo Martín Trápaga Sibaja, psicólogo capacitador del COESIDA.
En el año 2015, el Comisionado de Seguridad Pública, Vialidad y Protección Civil Municipal, José Luis Echeverría Morales, resaltó la importancia de dar seguimiento a este tipo de actividades que sin duda, contribuyen a la formación integral de los elementos de seguridad del Ayuntamiento capitalino.
“Hoy vemos un mayor interés de los elementos de seguridad pública en los talleres. Al principio, la mayoría desconocía la información básica sobre el VIH, el sida, las formas de transmisión e incluso, la forma correcta de colocar un condón; pero ahora, cada vez son más los que se suman al programa y además de transmitir el mensaje entre sus compañeros, lo llevan a sus hogares y eso es muy importante”, aseguró. Además de la participación del psicólogo Martín Trápaga Sibaja, las y los policías fueron capacitados por la médica Ángeles Pérez Silva y la psicóloga Angélica Castro Pineda, quienes los invitaron a ejercer su sexualidad de manera responsable y compartida.
Currently only half of people living with HIV globally are aware of their status. Of the remaining 50% many are not yet engaged in care, receiving antiretroviral therapy (ART) in a timely manner or – the ultimate goal of HIV treatment and prevention – achieving sustained viral suppression.
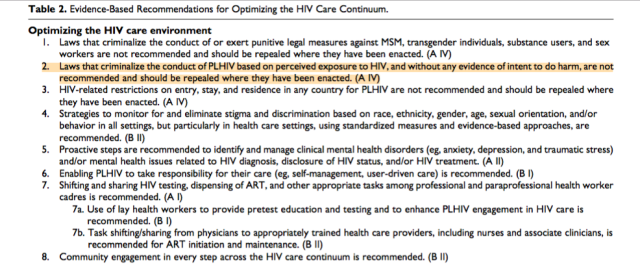
These new guidelines are the first to include HIV criminalisation as one of eight key critical barriers that prevent people living with HIV from enjoying both the therapeutic and preventive effects of ART.
In many settings, optimizing the HIV care environment may be the most important action to ensure that there are meaningful increases in the number of people who are tested for HIV, linked to care, started on ART if diagnosed to be HIV positive, and assisted to achieve and maintain long-term viral suppression. Overcoming the legal, social, environmental, and structural barriers that limit access to the full range of services across the HIV care continuum requires multistakeholder engagement, diversified and inclusive strategies, and innovative approaches. Addressing laws that criminalize the conduct of key populations and supporting interventions that reduce HIV-related stigma and discrimination are also critically important. People living with HIV also require support through peer counseling, education, and navigation mechanisms, and their self-management skills reinforced by strengthening HIV literacy across the continuum of care.
The full HIV criminalisation recommendation (Recommendation 2) is below.
Recommendation 2: Laws that criminalize the conduct of PLHIV based on perceived exposure to HIV, and without any evidence of intent to do harm, are not recommended and should be repealed where they have been enacted. (A IV)
Numerous countries have enacted laws that criminalize behaviors associated with HIV exposure, many of which pose a low or negligible HIV transmission risk. No differences in behavior have been noted between settings that enact such laws and those that do not. Many of these laws do not take into account measures that reduce HIV transmissibility, including condom use, and were enacted before the preventive benefit of ART or antiretroviral (ARV)-based preexposure prophylaxis (PrEP) was fully characterized. Most PLHIV who know their status take steps to prevent transmitting HIV to others.HIV-specific laws thus primarily exacerbate HIV-related stigma and decrease HIV service uptake.
Last week’s publication of the Norwegian Law Commission’s disappointing report was “a crucial moment for us in Norway – actually for all HIV activists in the Nordic countries,” says Kim Fangen, the only member of the Commission to vote against the use of a specific law to control and punish people with HIV and other sexually transmitted infections.
Kim’s alternative vision, as detailed in Chapter 10 of the report (only available in the full Norwegian version, not the English summary, but translated into English by the HIV Justice Network and included in full below) is one of a supporting and enabling environment, where people living with HIV are seen as part of ‘the solution’ and not ‘the problem.’
“It is not through criminal law that we reduce the spread of HIV,” he writes. “I believe that HIV and other sexually transmitted infections are solely a health issue. That’s where the focus should and must be, if one wants to prevent more infections. This means that we must change our mindset and change our course from criminal regulation to a health-related approach.”
His solution is a uniqely Norwegian version of the new paradigm of HIV prevention for people living with HIV, known as Positive, Health, Dignity and Prevention – a comprehensive approach to supporting people living with HIV with their prevention and social needs, not through fear or coercion but through empowerment and with dignity. Much of the solution is already there in Norway’s HIV Action Plan – but as Kim notes, with a few exceptions, little of the plan has actually been actioned.
Q: As the only person openly living with HIV on the twelve person Commission, what did you hope to achieve?
When I was asked to be asked to be part of the Norwegian Law Commission, I was very happy and proud. I, and many of my friends and colleagues living with HIV, believed it was a promising sign that they had reserved one of the Commission’s twelve seats for someone living with HIV.
I actually believed that there was a genuine will and desire to investigate the issues raised in our mandate and to produce recommendations that hopefully would point Norway in a new direction, towards decriminalising potential HIV ‘exposure’ and unintentional transmission.
I did not think that it would be easy, but I thought it would be possible. I honestly thought that finally there would be no need to single out people with HIV as group so hazardous that Norwegian society felt the need of a specific law to protect itself.
What I never envisaged was that, in the end, I would be standing alone.
Q: When did you realise that you point of view was not going to be supported by the rest of Commission?
It was quite early in the process. I realised that not only was it going to be difficult, but that I was quite alone not wanting a specific law.
I really feel that the reason for my inclusion on this Commission was not to learn more from those of us living with HIV, but was instead a kind of tokenism – by having a person living with HIV on board I believe they thought they would be able to silence us once and for all.
Q: What disappoints you the most about the report?
I cannot help feeling that a great opportunity has been lost and the goodwill of people with HIV misused. This is a sentiment I share with many of my friends and colleagues both at home and abroad. Many of us are so very disappointed. We honestly believed we would finally experience a change now, just as we, ironically, are about to commemorate 30 years since the first Norwegian was diagnosed with HIV.
And so I am afraid that we will not get the debate we so desperately need. I worry that this report will provide politicians with easy solutions, something Norway will not benefit from.
I’m glad that you pointed this out. I do feel that I have been listened to when I have spoken of supporting people living with HIV, and the clinics can do much more to help in guiding and strengthening each individual. This is the kind of work I am directly involved in myself.
Q: Do you think the report’s content and conclusions are completely consistent with Norway’s commitments to human rights and in terms of making laws based on evidence and not ideology?
No, I do not. I have on several occasions talked about our responsibility to practise what we preach. I do not think Norway is doing that.
Q: How might the report impact the rest of the Nordic region?
HIV and the law are being debated and discussed all over the Nordic region. All of the four countries are at different stages but our goals are the same, to end the overly broad criminalisation of HIV.
My hope is that Sweden, Denmark, Finland and Norway will join forces. We will be so much stronger if we pull together. Next year will we will be commemorating 30 years since Norway had its first HIV diagnosis. We, in the newly-established HIV Patient Network will be using that to the fullest and, of course, criminalisation will be on top of the list.
Q: The process will take another 18 months before parliament decides on whether or not to enact or abolish a specific criminal law. What are your plans?
My only hope now is that the international response to this report will be so substantial, so clear, and so loud that it will have an impact on Norway’s politicians.
I am hoping to organise a joint Nordic meeting in Oslo sometime during 2013, preferably before the deadline for the hearing letter goes out, when we are still able to influence the process before it is finalised some time in 2014.
If we can thoroughly examine the situation in all of the Nordic countries, invite politicians, medical and legal practitioners, experts and specialists in fields like sexuality, ethics and human rights, as well as members of the international civil society, we should be able to strengthen our arguments and support those in office who actually can directly influence the debate.
In the meantime, for those who haven’t already signed the Oslo Declaration on HIV Criminalisation, please take a moment to read it and support our efforts. I would like thank everyone who contributed, who made this possible, and especially to the HIV Justice Network. I know that it has already caused a stir in Norway, and I feel that there is so much more to gain from it. It’s like a tool that is still in its wrapping, and it has yet to reach its full potential.
Below is the full English translation of Kim’s submission to the Commission, outlining his alternative vision, from Chapter 10 of the report.
One of the committee members, Kim Fangen, lives with HIV and has been involved in working in this field for many years.
As stated during the assessments in Section 11.2.1.2, Mr Fangen says that there should be no special penal targeting disease transmission directly between humans. Mr Fangen believes that any criminal proceedings should take place using the general penalty provisions of bodily harm, and that these penal provisions should only be applied where the perpetrator acted with the intent to infect another, and the disease is transferred.
The rationale for this position is stated in the following that Mr Fangen has written on this matter:
New time. New inspiration.
HIV has been a part of our global reality for over 30 years. It is estimated that 60 million people have been infected during this period, 35 million of whom are alive today. For the first time in the history of HIV in the world, data show that the number of people that are newly diagnosed HIV positive is on a downward trend. This is primarily because many people with HIV have access to treatment. Treatment not only allows people with HIV to live a long healthy life, but the majority who are on treatment have a fully suppressed HIV viral load and are thus very unlikely to be infectious. The US Centers for Disease Control and Prevention (CDC) recently reviewed the latest research data and concludes that antiretroviral therapy reduces the risk of a person with HIV transmitting the virus to an HIV-negative person by 96%. UNAIDS has begun to talk about a world without HIV in its 2011-2015 strategic plan, ‘Getting To Zero’. Medical progress has thus changed the situation in a very positive direction. This change should also be reflected in legislation and case law.
However, the situation is not only positive. In some countries and in some groups, we are seeing an increase in the number of new HIV diagnoses. In Norway, the number of annual new HIV diagnoses among gay and bisexual men and other men who have sex with men has tripled since 2002. This increase is very serious and requires that we strengthen and develop prevention among both HIV-negative and HIV-positive individuals.
Does HIV belong in the criminal code?
As person living with HIV, my primary focus has been on HIV when the committee has discussed details of the currently adopted provisions for serious communicable infectious diseases in the 2005 Penal Code § § 237 and 238. Most of my arguments stem from the experiences we have had with HIV in the applicable provisions of the 1902 Penal Code § 155, which for years has rightly been called the ‘HIV paragraph’. As you know, this is not an HIV-specific law, but in practice it has, almost without exception, been used to prosecute HIV. There are only a few cases where it has been applied with another communicable disease (respectively, hepatitis B and hepatitis C).
I think that HIV-related work, both in terms of caring for people with HIV, and preventing new infections, has not well been served by such legislation, which stigmatises those of us with HIV and creates the perception that were are potential criminals, and does not take into account that people with HIV have the right to a good sex life. The legislation does not relate to the psycho-social challenges it means to live with HIV, and is not adapted to the fact that the reduced quality of life and difficulty in coping with safer sex are often intertwined. The legislation has not been clear on what constitutes unlawful sexual behaviour, and criminal liability is not consistent in relation to current knowledge about HIV and the risk of transmission.
Furthermore, I believe that the implementation of this legislation violates the fundamental principles of equality before the law. It seems as if the law is both random and unfair when only a few cases have been filed in recent years, despite the fact that several hundred people are diagnosed with HIV each year. It also seems unfair and counterproductive that all responsibility should rest on those of us who are familiar with our own HIV status, when we know that many are not aware of their own status and that new infections require HIV-negative individuals to choose to have unsafe sex.
In light of the increasing number of new HIV diagnoses among gay and bisexual men and other men who have sex with men, one can rightly ask what does that suggest for this law in terms of HIV prevention? My contention is that it has not served its purpose, whether viewed from a public health perspective or an individual prevention perspective. HIV is no longer a threat to public health, as one assumed it was going to be early in the 1980s. We have been aware of this for many years now. Even before effective treatment arrived, this was a fact. Nevertheless, it seems that the ‘epidemic’ mentality lingers in the minds of many people.
A public health perspective, however, is important when it comes to the spread of other communicable diseases through air, water and food. I have therefore, together with a committee unanimously decided that § 238 should be amended to apply only to such infections, see chapter 11 and the committee draft laws in Chapter 14
It is not through criminal law that we reduce the spread of HIV. I believe that HIV and other sexually transmitted infections are solely a health issue. That’s where the focus should and must be, if one wants to prevent more infections. This means that we must change our mindset and change our course from criminal regulation to a health-related approach. Both partners should be responsible for their own sexual health, but this should not be linked to punishment. I do not believe that criminal law is a suitable tool for regulating health-related behaviours. Using the Penal Code, however, can make it appear as if the Government has been pro-active on this issue when instead it actually creates a false sense of security.
Decriminalisation
I believe that one should not criminalise unprotected sex and consequently the transmission of sexually transmitted infections. In sexual relations between two equal partners who voluntarily decide to have sex, no heed is given to criminalisation / criminal law at home, regardless of whether HIV is transmitted or not. I believe that punishment should only be used in cases where you can prove that someone has intended to transmit a communicable disease and succeeded in doing this. Then the general provisions on bodily harm can be used, but in all other cases general laws on ‘offences against the person’ should not be used.
My suggestion therefore implies a clear decriminalisation, as I suggest that prosecutions should only occur where there is intent in the form of wilful intent and infection actually occurs. Transmission that occurs through dolus eventualis [recklessness] should, I suggest, not be prosecuted, even if infection actually occurs. This also applies to cases where there is only a negligent state of mind. If there has only been the potential for exposure, i.e. infection has not occurred, as I have already suggested, this should not be punished.
People with HIV – an untapped resource
Those of us who are living with HIV want to be involved in reducing infection rates. We want to be “part of the solution” and not be seen as a “problem”. Just as our society desires that all groups of patients are equal partners in health, I believe that people with HIV in particular are an important group to include. I think we are an untapped resource in prevention. We have unique knowledge in that can say something about why we were infected. This knowledge has so far not been made use of – no one asks us about possible underlying / contributory reasons why we were infected. Here, there is a great potential in terms of prevention of new infections, and we want to be involved in this work.
Common goals
Whatever we may think of the Penal Code as all actors within the HIV field (whether government, organisation or activist) a common goal is to prevent people from becoming infected with HIV.
How do we reach this goal? Measures should focus on the HIV-positive and HIV-negative. We must strengthen and set clear requirements for disease control. We need to improve the coping ability of all people living with HIV. We need more testing, more often. Those who are newly diagnosed who wish to start treatment should be allowed to do so. We need to focus on the importance of risk/harm reduction, and realise that it can make a substantial contribution to ‘traditional’ prevention. Doing even something right is better than doing nothing at all.
There is no reason that Norway might not become the best in the world in this area – we have the knowledge, skills and the economy. We have a clear situation, and we are able to reach everyone.
Sexually transmitted infections are a part of our shared reality. It’s not just HIV that is increasing in scope, but other infections. There are an increasing number of challenges, such as treatment-resistant gonorrhoea. We do not yet know the extent to which this will continue and what consequences will ensue. The more times a person is treated for a sexually transmitted infection, the greater the risk of complications or of developing resistance potentially resulting in a chronic condition. Although this information has reached the majority of the population it does not change the habit of having unprotected sex. We can surmise this from the ever increasing number of cases of sexually transmitted infections.
We should find a way to prepare a comprehensive plan as to how Norway should tackle all areas of sexual health. This plan must address both the dark and light sides of sexuality and must deal with sexuality throughout our life. Such a plan must aim to enhance the general population’s sexual health, while also dealing with special measures for vulnerable groups with special challenges, such as gay and bisexual men and other men who have sex with men, refugees, asylum seekers and their families.
This could be done by a committee that will have the mandate to prepare an action plan to enhance overall sexual health, including prevention of sexually transmitted infections. The current national strategic plan for improving sexual health is too one-sided by focusing on the prevention of unwanted pregnancies. Such a committee should have representatives of health authorities as well as representatives of relevant groups and relevant organisations.
National Action Plan
There are many HIV-positive people who believe that the National Action Plan ‘Acceptance and Coping, 2009-2014’ is a very important and appropriate plan for HIV prevention efforts. Here are six ministries and several agencies that are committed to comprehensive efforts in HIV-related work by defining objectives and strategic actions in a number of areas. Some of this is already implemented, but much remains to be done, and the recent mid-term conference showed that things are tough and that there is great frustration among the players.
What has been implemented includes the initiation of the first learning and activity courses for people with HIV. This course was developed through a partnership between The Health Information Centre and Department of Infectious Diseases, both at Oslo University Hospital, and the newly established Council for Patients with HIV has also contributed. Here, among other things, the mastery of sex life is an important part. This has been a successful pilot project that is supposed to be a constant for all who are living with HIV, and to all who are diagnosed with HIV, regardless of nationality, ethnicity and sexual orientation. We believe this is an important service for this patient group that until now has received little follow-up beyond the purely medical field. Another important measure implemented under the HIV plan is the training of health professionals who work with people with HIV to assist in their conversations with patients about changes in health-related behaviours, including sexual behaviour. The tool used is a method called motivational interviewing (MI) which increases the patient’s motivation to change. In 2011 almost 100 health professionals participated in such courses organised by the Directorate of Health. More such courses are needed, and these courses should be offered at different levels, so that MI is an integral part of care.
Such courses for both patients and healthcare providers is something that can increase both the efficacy and quality of life for people with HIV and are therefore very important health promotion and HIV prevention measures. Earlier initiation of treatment and increased focus on testing for HIV and other sexually transmitted infections are other measures that work to prevent new infections.
Apart from the above-mentioned exceptions, very few of the other parts of the HIV plan have been completed. Why has this happened? Why has this work come to a standstill? Why have we not managed to achieve several more goals outlined in the plan? Is it due to a lack of real will of the health authorities and other ministries to drive this plan forward? Have they declared themselves satisfied with making a good plan, and then delegated the responsibility for implementation to civil society and health care providers? Success requires national management and monitoring.
The way forward – a new tool offers new opportunities
I believe we have a unique opportunity now to show other countries how HIV and other sexual transmitted infections can and should be dealt with in a constructive and inclusive manner. By focusing on sexual health in general, and for the whole population, we could experience a reduction of HIV and other sexually transmitted infections. We must work to motivate and to inspire each individual and thus safeguard the best interests of society.
It’s a new era that should inspire all who live and work in this field. We know so much more now than when HIV was incorporated into the Penal Code. We have completely different opportunities today to fight this virus, by helping as many as possible to independently maintain their health. This is where we can help to reverse the negative trend we are experiencing nationally, and it will also give us an opportunity to show the way internationally. There are many eyes focused on Norway these days who are most interested in how we choose to move forward with this challenge. We have a responsibility to make this our opportunity to achieve the very best possible outcome.
You can select your preferred language from the 'Select Language' menu at the top of the page.
Continue
We use cookies to ensure that we give you the best experience on our website. By continuing to use our site, you are agreeing to our use of cookies. You can change your cookie settings at any time if you want. Find out more in our Privacy & Cookie Policy.




 In many settings, optimizing the HIV care environment may be the most important action to ensure that there are meaningful increases in the number of people who are tested for HIV, linked to care, started on ART if diagnosed to be HIV positive, and assisted to achieve and maintain long-term viral suppression. Overcoming the legal, social, environmental, and structural barriers that limit access to the full range of services across the HIV care continuum requires multistakeholder engagement, diversified and inclusive strategies, and innovative approaches. Addressing laws that criminalize the conduct of key populations and supporting interventions that reduce HIV-related stigma and discrimination are also critically important. People living with HIV also require support through peer counseling, education, and navigation mechanisms, and their self-management skills reinforced by strengthening HIV literacy across the continuum of care.
In many settings, optimizing the HIV care environment may be the most important action to ensure that there are meaningful increases in the number of people who are tested for HIV, linked to care, started on ART if diagnosed to be HIV positive, and assisted to achieve and maintain long-term viral suppression. Overcoming the legal, social, environmental, and structural barriers that limit access to the full range of services across the HIV care continuum requires multistakeholder engagement, diversified and inclusive strategies, and innovative approaches. Addressing laws that criminalize the conduct of key populations and supporting interventions that reduce HIV-related stigma and discrimination are also critically important. People living with HIV also require support through peer counseling, education, and navigation mechanisms, and their self-management skills reinforced by strengthening HIV literacy across the continuum of care.